Beyond Picky Eating: What Parents Need to Know About ARFID in Kids


- Avoidant/restrictive food intake disorder (ARFID) is an eating disorder that can show up in kids, and it may, at first, look like “picky eating.”
- However, ARFID is a diagnosable and often serious eating disorder, which develops out of sensory sensitivities, a lack of appetite or food interest, or a fear that something bad will happen from eating.
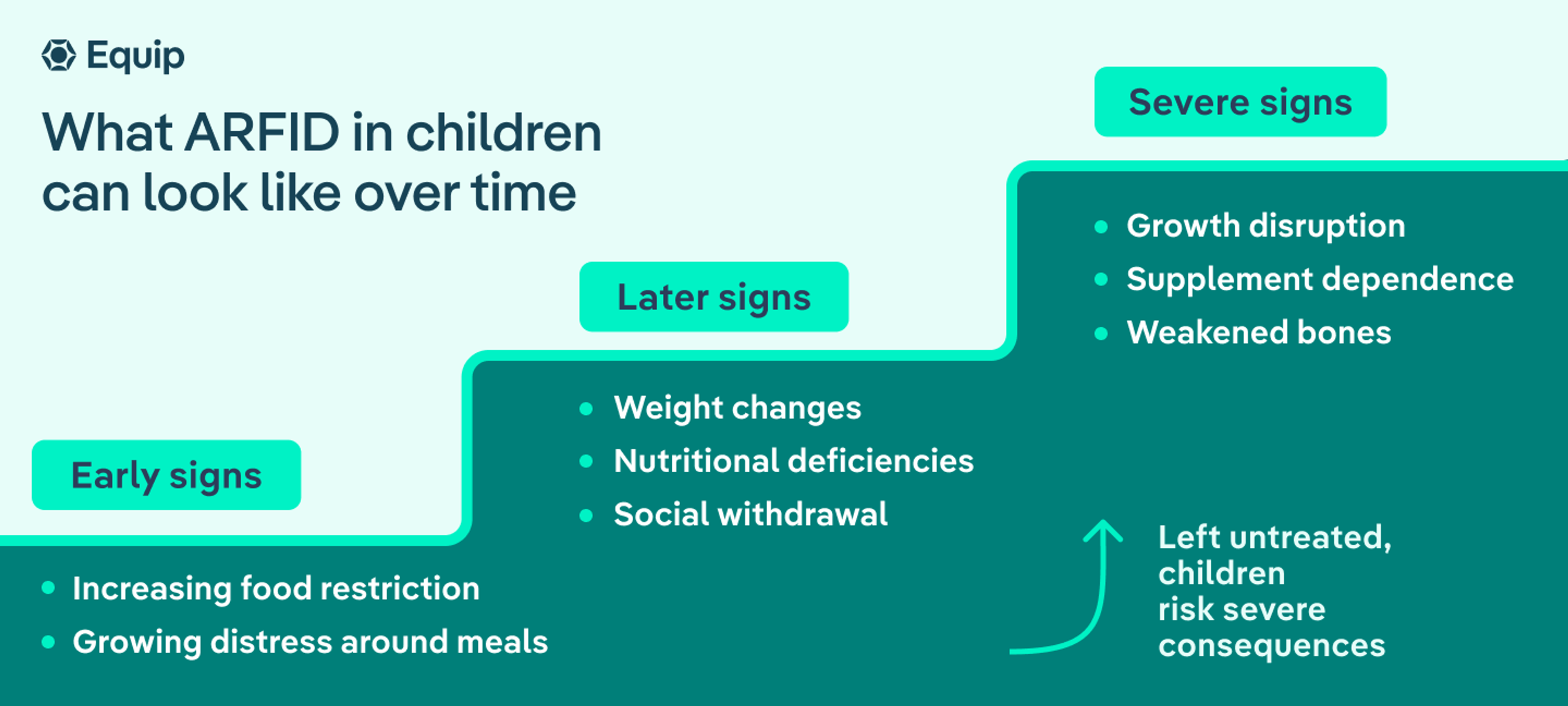
- When left untreated, the condition eventually leads to negative health effects by impacting normal growth and development and everyday functioning.
- Equip is the largest ARFID treatment provider in the U.S. and has a proven track record of helping people, including children, recover gradually and safely from ARFID.

If you’re a parent, maybe this scenario sounds familiar: Your child has been consistently refusing to eat any foods that make a “crunch.” At first, you chalk it up to the “picky eating” you remember from your own childhood, something that resolved over time as you tried more foods.
But then your child starts refusing to eat any foods that aren’t white or beige. And as the list of things they’re willing to eat grows shorter and shorter, your child starts losing weight or falling off their growth curve. That’s when you wonder if something else is going on. You worry about rotating the same five “safe” foods, which you know are not enough nutritionally, but your child’s distress when you encourage them to try new flavors feels unmanageable.
Behaviors like the ones described above indicate that something else is going on aside from typical picky eating. Yes, picky eating is a common childhood behavior, according to the Proceedings of the Nutrition Society—but it often fades as kids gain new experiences with food, whether at home, at school, or on playdates. Sometimes, though, seemingly picky eating can be an indicator of a serious condition.
Avoidant/restrictive food intake disorder (ARFID) is a recognized eating disorder in which a person eats a very small amount or variety of food (or both). Body image or weight concerns do not drive ARFID, though these issues often play a central role in other eating disorders.
Many factors can contribute to the development of ARFID in kids. But ARFID is not “just a phase,” and it is not your fault as a parent or caregiver, nor is it your child’s fault. And recovery is possible with the right support.
In this article, we explore ARFID symptoms in children, ARFID vs. picky eating, ARFID diagnostic criteria, and more.
What is ARFID?
ARFID is an eating disorder that is not driven by body image concerns or fear of weight gain. It develops out of sensory sensitivities, a lack of appetite or interest in food, or a fear that something bad will happen from eating or drinking certain items.
“Each of these reasons represents a presentation of ARFID,” says Michelle Jones, PhD, a licensed clinical psychologist and clinical instructor at Equip. “And people diagnosed with ARFID can experience one, two, or all three of these presentations. Importantly, individuals with ARFID do not restrict their intake due to body image distortions or a desire to lose or avoid gaining weight.”
ARFID was first defined in 2013 in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), which provides criteria for mental health diagnoses.
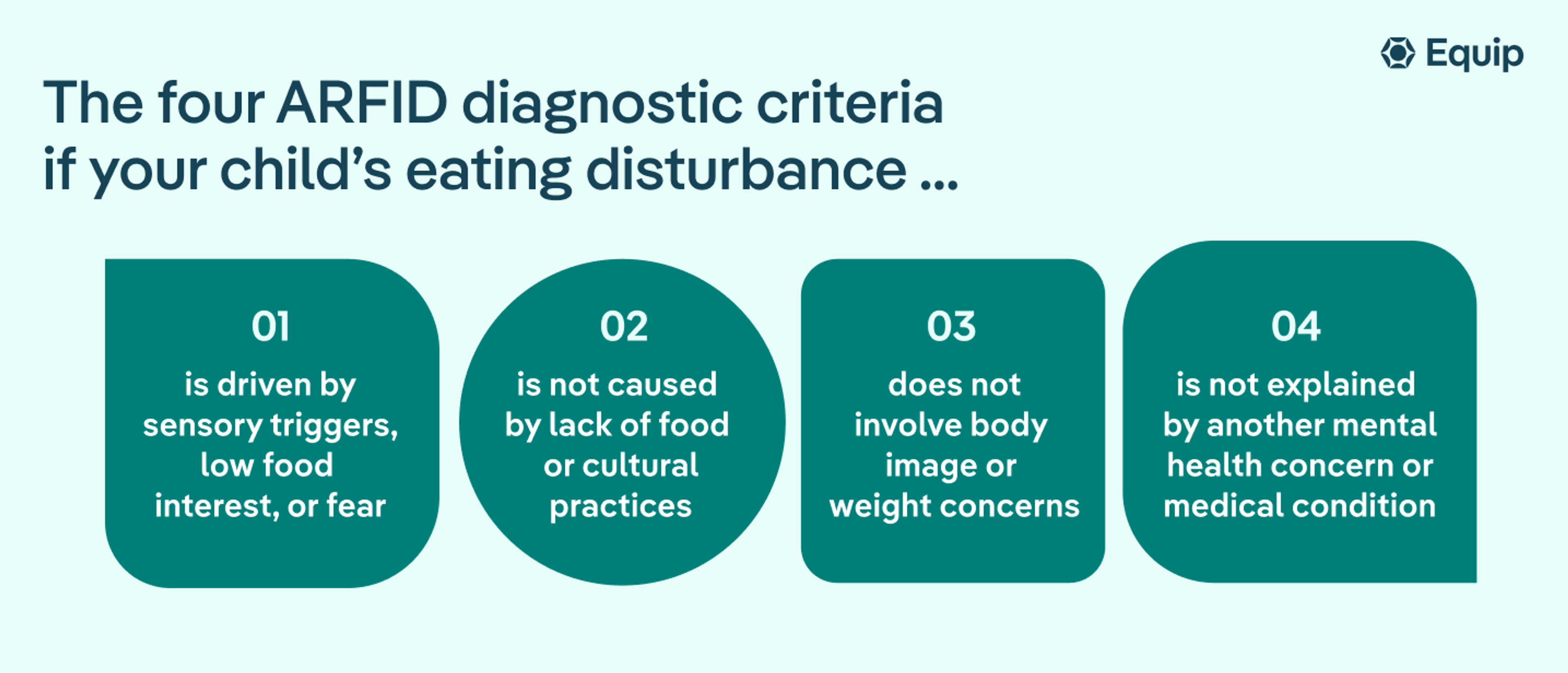
The four ARFID diagnostic criteria:
- Your child has an eating or feeding disturbance (e.g., sensory sensitivities, lack of food interest, or food fear) that leads to at least one of the following:
- Significant weight loss
- Significant nutritional deficiency
- Dependence on nutritional supplements (either orally or through a tube)
- Noticeable issues in social functioning
- The eating disturbance does not result from a lack of available food or a cultural practice.
- The eating disturbance does not involve body image or weight concerns.
- The eating disturbance is not explained by another mental health concern or medical condition.
ARFID is distinct from picky eating. It’s also not about stubbornness on your child’s part, nor is it some sort of parenting failure. Instead, ARFID results from underlying factors that are out of your control.
Determining the prevalence of ARFID in children is tricky. But, according to the Journal of Eating Disorders, it affects up to 15% of the population and often develops in childhood, though it can show up later in adulthood.
Is it ARFID or picky eating?
If your child is a difficult eater, understandably, you might be worried. Like many other parents and caregivers, you might find yourself in the position of having to determine whether what you’re picking up on is ARFID or more along the lines of normal childhood picky eating. The following table offers some clues.
Picky eating vs. ARFID in toddlers, children, or teens
Category | Typical picky eating | ARFID |
Range of foods accepted | Eats a limited number of foods but usually accepts at least one food from most food groups and may gradually try new foods | Eats an extremely restricted range of foods, sometimes only a handful of “safe” foods, with little willingness to expand diet |
Effect on growth or weight | Usually maintains expected growth, weight, and nutritional status despite food preferences | May experience weight loss, poor weight gain, growth delays, or nutrient deficiencies, or may require nutritional supplements |
Physical reactions to food | May complain about taste, texture, or appearance but generally does not have severe reactions | May gag, choke, vomit, or react in disgust or show anxiety when faced with certain foods |
Effect on daily life and social situations | Can usually participate in family meals, school lunches, parties, and restaurants with minor accommodations | Food avoidance significantly disrupts meals, school, travel, social events, family routines, or other daily activities |
Response to encouragement | May eventually try new foods with repeated exposure, positive reinforcement, or age | Encouragement, rewards, or pressure typically have little effect and may increase distress or avoidance |
What happens over time | Often improves naturally during childhood, with food variety expanding with age | Persists over time and may worsen without support or treatment; dietary restrictions remain severe |
ARFID and picky eating can look similar, especially at first, but the differences become clearer when eating patterns affect nutrition, growth, daily functioning, or overall well-being. For a more detailed breakdown, read our article on ARFID vs. picky eating.
Dr. Jones offers further insight to help illustrate the basic differences between the two. “When differentiating between ‘normative’ childhood picky eating and selective eating in ARFID,” she says, “I consider the child’s range of preferred foods, how stable those food preferences are over time, whether the child is becoming more limited in variety over time, and the impact of the limited variety on the child’s health and functioning.”
With picky eating, children typically eat at least a few foods from each of the five food groups, though they may have favorites or preferences for how those foods are prepared or presented. “A child with selective eating associated with ARFID may not be able to tolerate even minor changes in preparation or in sensory properties of foods without intervention,” Dr. Jones says.
Another key difference involves negative effects on health. “Generally, picky eaters will not experience significant negative impacts in terms of weight, health, or psychosocial functioning as a result of their eating habits,” Dr. Jones explains. However, children with ARFID eventually experience one or more of these health concerns.
What are the three presentations of ARFID?
ARFID shows up in three distinct ways, but many people with ARFID display characteristics of more than one.
- Sensory sensitivity: Your child avoids foods because of specific textures, tastes, smells, colors, temperatures, or general appearance. Maybe your kid dislikes when any of their foods touch on their plate. Or maybe they gag when you serve anything green.
- Low interest in food: Your child says they aren’t hungry or doesn’t show interest in food. In teens, low interest may show up as forgetting to eat. Younger kids may not show any pleasure in foods that kids typically enjoy, and dinnertime might always feel like a battle where you’re trying to get them to eat anything.
- Fear of aversive consequences: Your child might fear throwing up or choking if they eat specific foods or eat in general. This presentation of ARFID may develop after a frightening experience with food. For example, after an incident in which food got stuck in the back of their throat at a birthday party, they may refuse to eat anything that isn’t pureed or liquefied.
What are the signs of ARFID in children?
ARFID can have both behavioral and physical symptoms. As a parent or caregiver, you might be more aware of the behavioral signs of ARFID in your kid, while other signs might show up at the doctor’s office. Here’s a breakdown of ARFID symptoms in children.
Behavioral signs
The behavioral signs of ARFID in kids might show up at home, school, or during social events, such as playdates, birthday parties, or larger family gatherings. Often, they occur in all these settings.
Your child might have ARFID if they:
- Eat only a small number of foods, refusing all others
- Continue to adamantly refuse certain foods even after gentle encouragement to try new flavors or textures
- Reject entire food groups (such as fruits or dairy)
- Get upset when designated “safe” foods aren’t available
- Display fear of choking or throwing up from eating
- Have emotional reactions to food, whether crying or panicking, especially when pressured to eat
- Eat noticeably slower than other people
- Refuse to eat at restaurants or in social situations
- Require you to bring “safe” foods to events
- Routinely skip meals or refuse to eat altogether
Physical signs
You might also notice physical signs that are consistent with ARFID. These symptoms could also come to light during a visit to your pediatrician.
Your child might have ARFID if they experience:
- Poor weight gain for their age
- Unexplained weight loss, especially when they should be gaining as part of their development
- Vitamin, mineral, or other nutrient deficiencies that show up through testing
- Thinning hair or pale skin
- Low energy or unusual fatigue from not eating enough
- Delayed puberty
- Digestive issues, such as constipation from not getting enough fiber
- Dependence on nutritional supplements, such as meal-replacement drinks
- Dehydration symptoms
How does ARFID affect a child’s health?
ARFID can affect both physical and mental health in a variety of ways. Nutritional deficiencies are just some of the potential impacts that may show up, while others result from extreme anxiety about food.
Common nutrient deficiencies in ARFID and what they might look like:
Nutrient deficiency | Why it matters | Possible signs parents may notice |
Iron | Supports healthy red blood cells and oxygen delivery throughout the body. | Fatigue, low energy, pale skin, difficulty concentrating, poor school performance, headaches |
Calcium | Essential for bone growth and strength during childhood and adolescence. | Delayed bone development, increased risk of fractures, bone pain, dental issues |
Vitamin D | Helps the body absorb calcium and supports bone and immune health. | Bone weakness, muscle aches, delayed growth, frequent illnesses |
Zinc | Plays a key role in growth, immune function, and wound healing. | Slowed growth, poor appetite, frequent infections, slow wound healing |
Protein | Needed for growth, muscle development, and tissue repair. | Poor weight gain, loss of muscle mass, slowed growth, low energy |
Vitamin B12 | Supports nerve function and red blood cell production. | Fatigue, weakness, difficulty concentrating, numbness or tingling in severe cases |
Vitamin C | Helps support immunity, wound healing, and iron absorption. | Easy bruising, bleeding gums, slow wound healing, frequent illness |
Fiber | Supports digestive health and regular bowel movements. | Constipation, stomach discomfort, irregular bowel habits |
Healthy fats | Important for brain development, growth, and energy needs. | Poor weight gain, difficulty meeting calorie needs, low energy levels |
Growth and development risks
Growth and development disruption is one of the key factors that help healthcare providers distinguish ARFID from picky eating. If your pediatrician has concerns, they may evaluate your child for ARFID or other conditions. However, if you notice issues with growth or development, you can always talk to your provider about what might be going on.
Growth and development concerns include:
- Height and weight percentiles may drop on growth charts
- Puberty may be delayed, which can delay other types of development
- Muscles do not develop, leading to difficulty with everyday activities and play
- Bone health suffers, leading to potential fractures
- Immune system issues may lead to more frequent or severe illness or trouble with wound healing
- Energy levels can be low, causing trouble with general functioning
Social and emotional effects
The rigidity around food that is present in ARFID, and the resulting nutritional deficiencies, can also lead to social and emotional issues.
Social and emotional effects include:
- Poorer performance in school
- Difficulty concentrating or paying attention
- Low energy for participating in activities
- Social avoidance, including for birthday parties, playdates, school outings, extracurriculars, etc.
- Anxiety when eating in public
- Trouble engaging with family at meals
What conditions commonly occur alongside ARFID?
Several conditions are associated with ARFID, though just because your child has one of the following conditions does not automatically mean they have ARFID, or vice versa. The conditions just share similarities, and may drive one another.
For example, sensory concerns are sometimes a symptom of autism spectrum disorder (ASD), which may lead to food-texture aversions, according to the journal Current Opinion in Psychology.
Likewise, a lack of hunger cues is associated with attention deficit/hyperactivity disorder (ADHD), according to Current Psychiatry Reports. This is partly because of how the condition affects the brain, and also because treatment medications can suppress appetite.
Additionally, obsessive-compulsive disorder (OCD) may contribute to the fear of certain foods, according to the journal European Eating Disorders Review.
Common ARFID comorbidities:
- Anxiety disorders
- Attention deficit/hyperactivity disorder
- Autism spectrum disorder
- Gastrointestinal disorders (e.g., irritable bowel syndrome or gastroesophageal reflux disease)
- Obsessive-compulsive disorder
- Sensory processing disorder
How is ARFID diagnosed in children?
ARFID is diagnosed in children after a thorough evaluation from a pediatrician or other clinician. When you take your child to see their doctor, here’s what might occur.
They may:
- Ask about your child’s symptoms or how they act around food.
- Ask about or reflect on your child’s medical history to see if their symptoms could be attributed to another medical concern.
- Ask about your child’s life experiences, such as whether they’ve experienced trauma or a traumatic food-related incident.
- Ask about your child’s overall mental health, since anxiety or another condition may be a contributing factor to their behavior surrounding food and eating.
- Ask about family medical history, since ARFID can have a genetic component.
- Evaluate whether your child’s growth and development are consistent with other children their age.
- Perform a blood draw to test for nutrient deficiencies.
- Perform allergy testing to confirm or rule out food allergies or sensitivities.
Keep in mind that ARFID is a lesser-known eating disorder, despite how common it is. So a provider might not notice the condition or might even dismiss your concerns as being just “normal picky eating” that your child will recover from with age. That’s why seeing an ARFID-informed provider is crucial if you continue to have concerns that your child has the condition or another potential eating disorder. Equip’s free ARFID quiz can be a helpful place to start.
When to contact your child’s doctor
If you have concerns about your child’s eating habits, whether you suspect picky eating or ARFID, never hesitate to reach out to their pediatrician or other provider for an evaluation.
“If symptoms that are associated with ARFID are causing a child significant problems in daily life, it’s a good time to seek help,” Dr. Jones says. “Specifically, professional guidance and treatment would be warranted if a child is experiencing weight loss or lack of appropriate growth or weight gain, problems functioning in daily life, significant distress, or any concerning medical symptoms related to poor nutrition.”
How is ARFID treated in children?
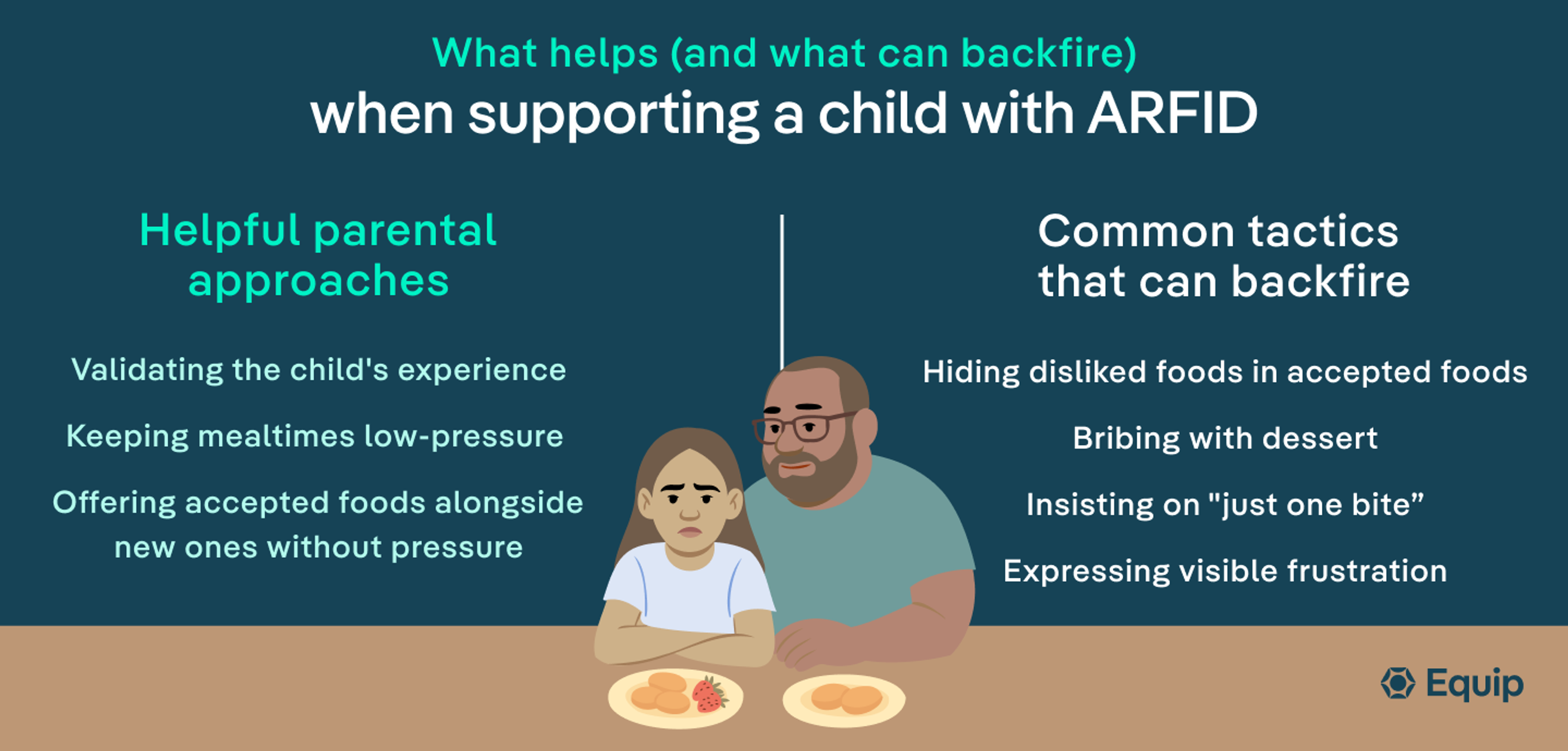
ARFID treatment in children usually involves family members and takes a gradual approach to addressing specific ARFID symptoms.
“Most treatment approaches start with helping the child and their caregivers understand what ARFID is and why it’s important to work on eating enough food and a wider variety of foods,” Dr. Jones says. “For children who are selective eaters, they will practice trying small tastes of new foods several times before gradually working on incorporating new foods that they are able to tolerate into their regular diet.”
Treatment may look a bit different if your child has low interest in food rather than specific aversions. “Interventions will involve making food more interesting and eating on a more regular schedule to ensure the child is eating an appropriate volume of food,” Dr. Jones explains.
Finally, if your child has fears around food, your care team may take another approach. “Children who are afraid of something bad happening during or after eating, such as vomiting or choking,” Dr. Jones says, “will practice facing their fears in small, achievable ways that gradually increase in difficulty until their fears decrease and they no longer interfere with the ability to eat.”
Working with a multidisciplinary care team helps set your child up for recovery. An ARFID-informed care team may use specific treatment methods, such as the following, some of which Dr. Jones described above:
- Exposure and response prevention (ERP) gradually exposes your child to triggers and helps them alter their response.
- Family-based treatment-ARFID (FBT-ARFID) actively includes parents and caregivers, empowering them to help manage their child’s nutritional recovery, while helping to remove stigma or feelings of blame and guilt.
- Cognitive behavioral therapy-ARFID (CBT-ARFID) addresses underlying food, sensory, or fear triggers while helping to normalize eating routines and expand food variety and overall intake.
The bottom line
ARFID is a recognized eating disorder that often develops in childhood or may show up later in life. One way it is distinct from pick eating is that it leads to negative health issues with growth and development and everyday functioning.
If you are concerned about your child’s eating habits or are wondering why they won’t eat and are losing weight, talking to a knowledgeable provider is a good idea. The hopeful news is that help is available and recovery is possible.
Equip offers individualized, evidence-based ARFID treatment for kids and can coordinate with external clinicians as needed. Schedule a call here to get started.
FAQ
Can a child have ARFID without autism?
Yes, a child can have ARFID even if they do not have autism spectrum disorder. The two conditions are associated with each other, but they also occur independently.
Can a child outgrow ARFID without treatment?
ARFID is a recognized eating disorder. It is not something a child will simply “outgrow” without treatment. ARFID is different from picky eating, which typically resolves as children try new foods over time.
Can ARFID cause a child to lose weight or stop growing?
Yes, ARFID can cause a child to lose weight or hinder their growth and development. The condition can lead to not eating enough to support developmental needs, and it can lead to nutritional deficiencies that impact overall health and well-being.
D’Adamo, Laura, et al. “Prevalence, Characteristics, and Correlates of Probable Avoidant/Restrictive Food Intake Disorder among Adult Respondents to the National Eating Disorders Association Online Screen: A Cross-Sectional Study.” Journal of Eating Disorders, vol. 11, no. 1, Dec. 2023, p. 214.
Keski-Rahkonen, Anna, and Anu Ruusunen. “Avoidant-Restrictive Food Intake Disorder and Autism: Epidemiology, Etiology, Complications, Treatment, and Outcome.” Current Opinion in Psychiatry, vol. 36, no. 6, Nov. 2023, pp. 438–42.
Taylor, Caroline M., and Pauline M. Emmett. “Picky Eating in Children: Causes and Consequences.” The Proceedings of the Nutrition Society, Nov. 2018, p. 1.
Thomas, Jennifer J., et al. “Avoidant/Restrictive Food Intake Disorder: A Three-Dimensional Model of Neurobiology with Implications for Etiology and Treatment.” Current Psychiatry Reports, vol. 19, no. 8, Aug. 2017, p. 54.









