ADHD and ARFID: Why Eating Can Feel So Hard — And What Actually Helps


- ADHD and ARFID can both make eating feel difficult, but they aren't the same thing. Some people experience one condition, while others experience both.
- Challenges like forgetting to eat, relying on safe foods, and low appetite aren't signs of laziness or a lack of willpower. Instead, they can be connected to how the brain processes food, hunger, and daily tasks.
- ARFID is more than picky eating. It is an eating disorder that involves restrictive eating and can affect nutrition, growth, health, or everyday life, and it's not driven by body image concerns.
- ADHD-related eating challenges are often inconsistent and situational, while ARFID typically involves more persistent food avoidance and impairment.
- Support can help. Treatment for concurrent ADHD and ARFID often includes a combination of strategies that make eating feel more manageable.

If you've been searching for answers about ADHD and ARFID, chances are eating feels harder for you than you think it should.
Maybe you've looked up at the clock and realized it's 4 p.m. and you haven't eaten all day. Maybe your child will eat only a handful of foods because certain textures, smells, or tastes make eating feel overwhelming. Or perhaps meal planning and food prep feel impossible to keep up with.
If that sounds familiar, you're not alone.
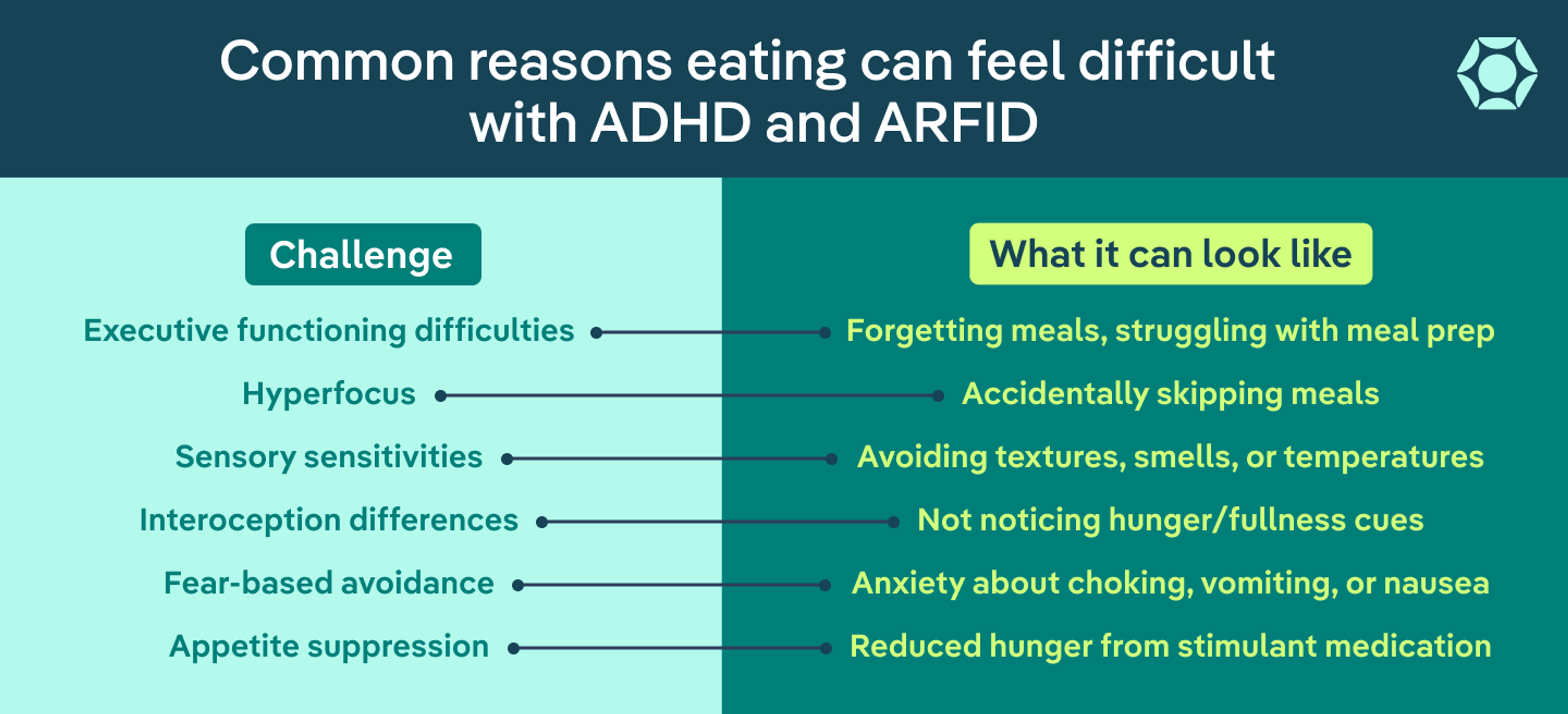
Many people with attention-deficit hyperactive disorder (ADHD) struggle with eating. They may forget meals, hyperfocus through hunger, lose their appetite on stimulant medications, or find the daily task of feeding themselves surprisingly difficult to manage.
For some, those challenges are related to ADHD itself. For others, they may be signs of avoidant/restrictive food intake disorder (ARFID), an eating disorder characterized by restrictive eating that's not driven by body image concerns.
The overlap between ADHD and ARFID can be confusing. Many people spend years wondering whether they're just picky eaters, bad at feeding themselves, or somehow lacking willpower. In reality, these struggles often stem from differences in how the brain processes hunger, sensory input, food, and daily tasks.
In this article, we’ll explore where ADHD and ARFID overlap, how they're different, and what effective treatment can look like.
Understanding ADHD, ARFID, and why they're often connected
ADHD is a neurodevelopmental condition that affects attention, impulsivity, activity levels, and executive functioning (the mental skills that help us plan, organize, remember, and follow through on tasks). It affects as many as 32% of children and 21% of adults. When it comes to eating, ADHD can make it harder to:
- Notice hunger cues
- Remember meals
- Plan and prepare food
- Shift attention away from a task long enough to eat
ARFID is an eating disorder characterized by restrictive eating that isn't driven by body image concerns. People with ARFID eat a very small amount or variety of food (or both), and this can lead to nutritional deficiencies, weight or growth concerns, distress around food, and difficulties in everyday life. There are different types of ARFID, but common reasons for food avoidance include sensory sensitivities, food-related fears, and a lack of interest in eating.
Although ARFID is often thought of as a childhood condition, it can affect people of all ages. Research suggests it may affect up to 15.5% of children and teens, while an estimated 0.3% of adults have the disorder. That latter number doesn’t tell the whole story, though: ARFID is often overlooked in adults, so many adults with ARFID have spent years struggling with food without realizing there's a name for what they're experiencing.
At first glance, some ADHD and ARFID symptoms can look similar. And an overlap between the two conditions is fairly common: One study found that nearly 17% of children with ARFID also had ADHD, while another reported rates closer to 1 in 4.
“It’s not always possible to differentiate between eating challenges associated with ARFID and those associated with ADHD,” says Michelle Jones, PhD, a clinical instructor at Equip. “However, it’s important to be aware of the challenges that can arise when individuals experience symptoms of both ARFID and ADHD, and adjust treatment goals and approaches to manage both.”
ADHD vs. ARFID: How to tell the difference
ADHD and eating disorders like ARFID are not the same thing.
But because of their similarities, telling them apart isn't always easy—and many people experience both at the same time. For example, someone might forget meals because of ADHD while also avoiding certain foods because of sensory sensitivity ARFID.
Still, there are a few ways they often differ, including:
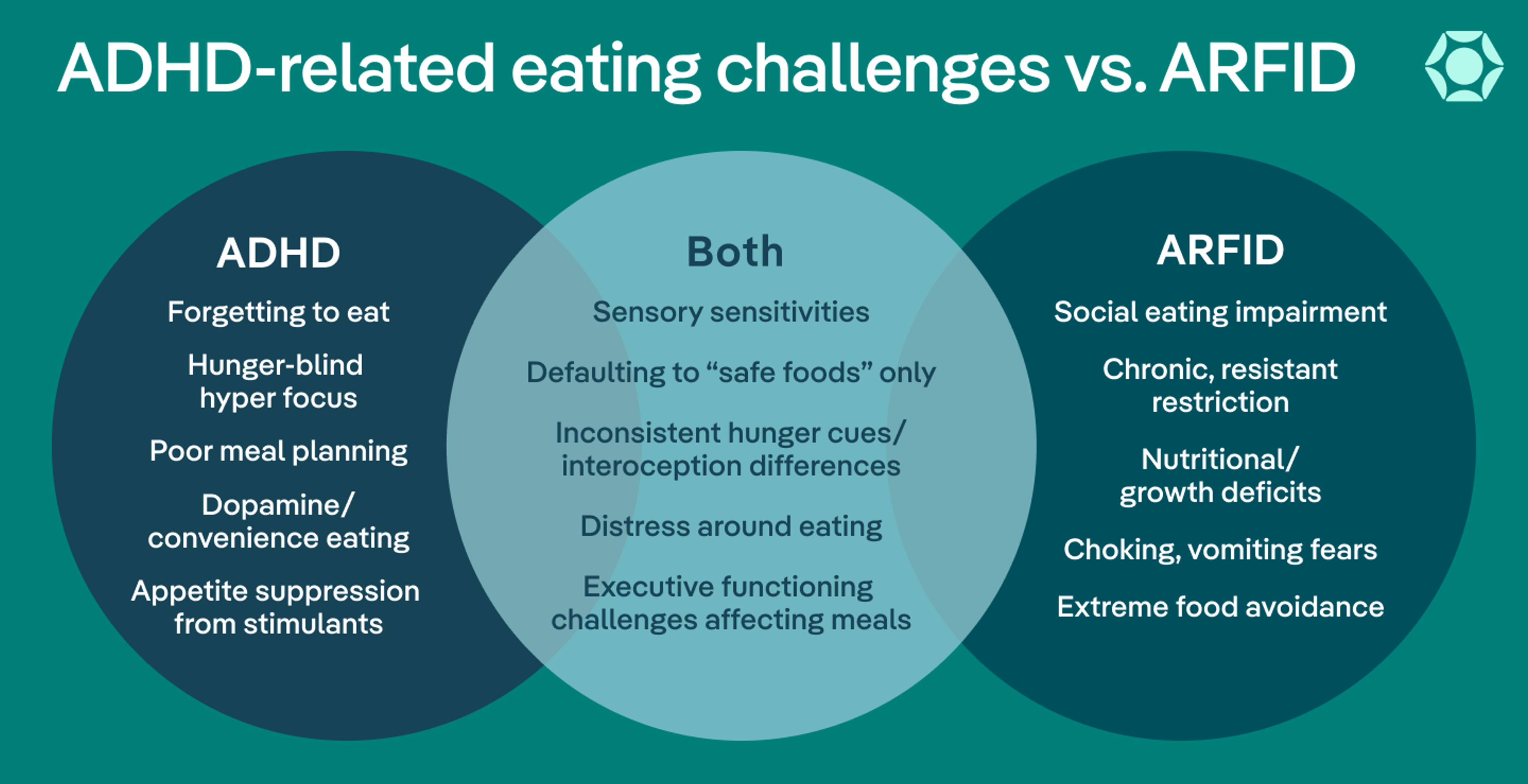
- The reason why eating feels difficult: ADHD food issues are often tied to distraction, hyperfocus, executive functioning difficulties, or appetite changes. ARFID-related eating challenges are more often driven by sensory sensitivities, low interest in food, or fear of choking, vomiting, or other negative consequences.
- Consistency of symptoms: Not eating with ADHD tends to be more situational. You might forget to eat one day and eat normally the next. ARFID-related food avoidance is usually more persistent.
- The reason behind food avoidance: People with ADHD may stick to familiar foods because they're convenient, predictable, or easy to prepare. People with ARFID often avoid foods because they feel overwhelming, distressing, or unsafe.
- Response to structure and support: Eating with ADHD may feel easier with the help of consistent reminders, routines, or easy-to-access meals. Someone with ARFID may continue struggling even with structure because the food itself feels difficult to eat.
- Impact on health and daily life: ADHD eating habits don't always cause significant nutritional, medical, or social consequences. ARFID is more likely to affect nutrition, growth, physical health, or participation in everyday activities.
ADHD Eating Challenges vs. ARFID vs. Both
Feature | ADHD-related eating challenges | ARFID | Co-occurring ADHD + ARFID |
Primary reason eating feels difficult | Executive functioning challenges, distraction, hyperfocus, inconsistent hunger cues | Strong aversions,, eating-related fears, or low interest in eating | Combination of executive functioning challenges and restrictive eating, sensory sensitivities |
Common eating patterns | Forgetting meals, grazing, irregular eating patterns, relying on convenience foods | Strong food avoidance, limited safe foods, distress around unfamiliar foods | Forgetting meals plus highly restricted food choices |
Flexibility around foods | Often able to eat alternatives with reminders, support, or planning | Limited flexibility; unfamiliar foods may feel overwhelming or unsafe | Executive functioning challenges make existing food restrictions harder to manage |
Response to routines and reminders | Eating often improves with reminders, routines, or easier food access | Restriction typically persists even with structure | Some improvement with structure, but food avoidance and distress remain significant |
Sensory issues or fear around food | May dislike certain textures or tastes, but can often adapt | Sensory distress or fear strongly drives food avoidance | Sensory challenges combined with ADHD overwhelm or hyperfocus can reinforce restriction |
Nutritional or medical impact | May lead to skipped meals or inconsistent nutrition | Can lead to nutritional deficiencies, weight or growth concerns, and other health complications | Higher risk of inadequate nutrition because challenges overlap |
What daily life may look like | Skipping meals while hyperfocused, struggling with meal planning, forgetting to eat | Eating only a small number of safe foods, avoiding social eating situations | Safe foods, skipped meals, sensory overwhelm, and difficulty maintaining eating routines |
Why ADHD and ARFID often occur together
ADHD doesn't cause ARFID. But some ADHD traits can make restrictive eating more likely (or make existing eating challenges harder to manage), including:
- Sensory sensitivity: Certain textures, smells, tastes, or appearances of food can feel intensely uncomfortable or overwhelming, which is why ADHD and food aversions sometimes overlap.
- Executive functioning challenges: Planning meals, grocery shopping, preparing food, and remembering to eat all require executive functioning skills. Because ADHD can make these skills more challenging, food-related tasks may require more effort and mental energy than people realize.
- Differences in hunger and fullness cues: Many people with ADHD struggle to consistently recognize or respond to these cues, making it harder to keep up regular eating patterns. (This is one reason why ADHD and binge eating disorder can also overlap.)
- Anxiety and food-related fears: People with ADHD are more likely to experience anxiety, which can amplify concerns around eating. At the same time, a negative experience with food, intense sensory discomfort, or fears around eating can lead to increasing food avoidance over time.
- Appetite suppression from medication: ADHD and appetite changes can go hand in hand, especially for people taking stimulant medications. These medications can reduce hunger, making it harder to eat enough throughout the day.
- Neurodivergence: ADHD, autism, and other neurodevelopmental differences are more common among people with ARFID, which may help explain why so many people see themselves in both experiences.
Signs it may be time to seek help
Many people with ADHD, ARFID, or both spend years wondering whether their eating challenges are "serious enough" to deserve support.
But you don't have to wait until things feel extreme to ask for help. If eating is causing stress, affecting your health, or getting in the way of daily life, then it's worth talking to a healthcare professional.
Some signs it may be time to seek support include:
- Weight loss or poor growth: Restrictive eating can make it difficult to get enough energy and nutrients to support growth, development, and overall health.
- Nutritional deficiencies: A very limited diet can increase the risk of missing important nutrients, especially when you avoid entire food groups.
- Fatigue, dizziness, or fainting: These can be signs that your body isn't getting the nutrition it needs.
- Increasing food restriction: The list of foods that feel "safe" continues to get smaller over time.
- Distress around eating: Meals, snacks, restaurants, social events, or trying new foods regularly cause anxiety, frustration, or overwhelm.
- Social or family impact: Eating challenges are affecting relationships, school, work, travel, or social activities.
- Reliance on supplements or meal replacements: Nutritional supplements can be helpful in some situations. But relying on them because eating feels too difficult may be a sign that it’s time to seek support.
Most importantly, trust your experience. You don't need to prove that your struggles are severe enough to deserve help. If food, eating, or nutrition feels like a constant source of stress, that's reason enough to start a conversation.
What treatment for ADHD and ARFID can look like
The good news is that support is available, and you don't have to figure it out on your own. Because ADHD and ARFID can affect eating in different ways, treatment often works best when it addresses both the eating challenges and the reasons behind them.
Many people benefit from working with a multidisciplinary team of professionals—like a therapist, dietitian, physician, and psychiatrist—who can help address different aspects of recovery.
Depending on a person's needs, treatment may include:
- Therapy: Therapy can help you better understand your relationship with food, manage anxiety, build coping skills, and gradually work through food-related fears.
- Nutrition support: A dietitian can help you build a more varied diet, address nutritional deficiencies, and develop eating strategies that fit your needs.
- Medical monitoring: Regular medical care can help identify and address complications such as nutritional deficiencies, weight loss, growth concerns, or other health issues.
- Exposure-based approaches: ARFID treatment often includes gradual exposure to feared or avoided foods. Over time, this can help food feel less overwhelming or distressing
- Sensory accommodations: Treatment may include honoring safe foods, adjusting food preparation methods, or finding ways to reduce sensory overwhelm while gradually building flexibility.
- Executive functioning supports: Reminders, visual schedules, easy-to-prepare foods, and other practical tools can make eating feel more manageable for people with ADHD.
- Family involvement: For children and teens, caregivers often play an important role in creating a supportive, low-pressure eating environment and helping treatment strategies carry over into daily life.
- Medication coordination: For people taking ADHD medication, treatment may involve working with healthcare providers to address appetite suppression or other medication-related eating challenges. “It may [also] be necessary to eat at times when you don’t feel hungry to ensure that you are eating enough and helping your body regulate hunger cues as much as possible,” adds Jones.
Treatment is most effective when it meets you where you are. With the right support, many people are able to expand their food options, reduce stress around eating, and feel more confident navigating meals, social situations, and everyday life.
The team at Equip—the largest ARFID provider in the U.S.—can help you start on your ADHD and ARFID treatment journey (as a first step, it may be helpful to take Equip’s free ARFID self-screener).
Tips for daily life
“Managing ARFID symptoms when you have ADHD may require specific strategies or supports to manage challenges related to executive functioning, sensory processing, or interoceptive awareness,” says Jones.
Just remember: What works for someone else may not work for you. The best approach is often the one that feels realistic, sustainable, and supportive of your individual needs.
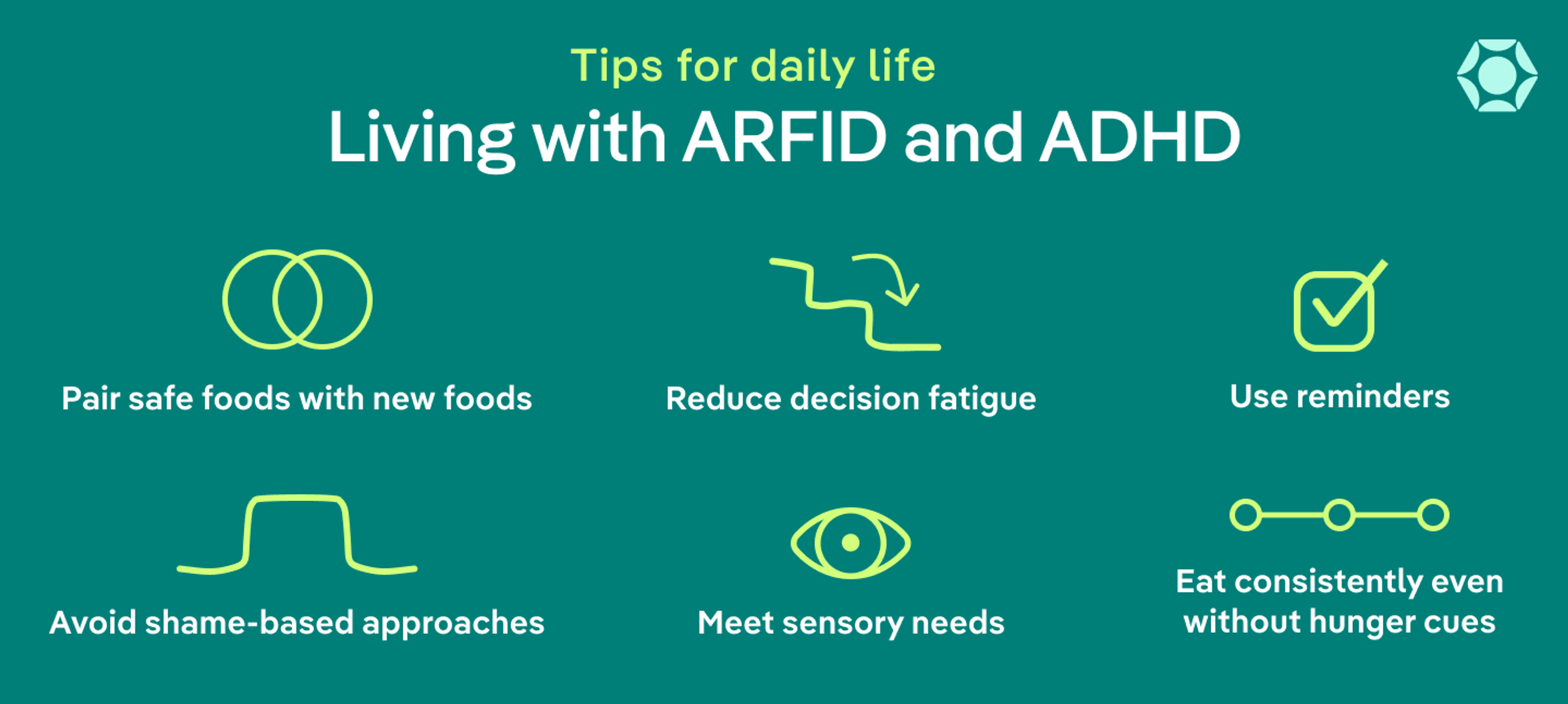
Here are some strategies Jones recommends:
- Optimize your environment: Eating can be easier when your environment works for you. That might mean reducing sensory distractions, such as loud noises or visual clutter, or adding sensory input that helps you stay engaged, such as listening to music or sitting in a more comfortable position.
- Use external reminders: Visual timers, phone alarms, calendar notifications, meal guides, or other cues can help if you tend to forget meals or lose track of time.
- Ask for support when you need it: Friends, family members, or caregivers may be able to help with meal planning, grocery shopping, food preparation, or creating a more supportive eating environment.
- Don't rely on hunger alone: If your hunger cues are inconsistent or medication suppresses your appetite, you may need to eat on a schedule (sometimes referred to as “mechanical eating”) rather than waiting until you feel hungry.
- Build awareness of hunger and fullness: Checking in with your body before and after meals, practicing mindfulness, or tracking hunger and fullness cues can help strengthen interoceptive awareness over time.
- Accommodate sensory needs: Small adjustments—such as changing a food's temperature, texture, or preparation method—can sometimes make meals feel more comfortable and approachable, even if they don’t include an ADHD food fixation or ARFID “safe” food.
- Practice self-compassion: Struggling with food isn't a personal failure. Approaching your food-related challenges with curiosity rather than criticism can make it easier to identify what helps and advocate for the support you need.
The bottom line
For people with ADHD, ARFID, or both, eating challenges are often about much more than food. Sensory sensitivities, executive functioning difficulties, inconsistent hunger cues, and food-related fears can all play a role, among other factors.
Whatever the reason, struggling with food is not a personal failure. You deserve support that helps you understand your needs, meet your nutritional goals, and feel more confident around food.
Frequently Asked Questions (FAQs)
Can adults have ADHD and ARFID?
Yes. While ADHD and ARFID are often discussed in children, both conditions can affect adults as well. Some adults have lived with eating challenges for years without realizing there may be an underlying explanation, and the same can be true of ADHD. Others may develop ARFID later in life after a negative food-related experience, illness, or an increase in sensory sensitivities.
Do ADHD medications make ARFID worse?
For some people, stimulant medications can reduce appetite, making it harder to eat enough throughout the day. While ADHD medications don't cause ARFID, appetite suppression can sometimes make existing eating challenges more noticeable or more difficult to manage. If you're concerned about changes in appetite, talk with your healthcare provider.
Is ARFID a lifelong condition?
Not necessarily. Everyone's experience is different. With appropriate support, many people are able to expand their food variety, reduce anxiety around eating, and improve their nutritional intake. Progress often takes time, but treatment can absolutely help make eating feel more manageable.
Che, Yunqiu et al. “Avoidant/Restrictive Food Intake Disorder in Adult Patients with Gastrointestinal Diseases: A Concept Analysis Using Evolutionary Approach.” Risk management and healthcare policy vol. 18 2063-2080. 21 Jun. 2025, doi:10.2147/RMHP.S520802
Cucinotta, Ugo et al. “A Systematic Review to Manage Avoidant/Restrictive Food Intake Disorders in Pediatric Gastroenterological Practice.” Healthcare (Basel, Switzerland) vol. 11,16 2245. 10 Aug. 2023, doi:10.3390/healthcare11162245
da Fonseca, Pâmela Gracielle et al. “The influence of family in children's feeding difficulties: an integrative review.” Frontiers in pediatrics vol. 13 1609714. 9 Jul. 2025, doi:10.3389/fped.2025.1609714
Finn, Daphna M et al. “Pharmacotherapy for attention deficit/hyperactivity disorder in youth with avoidant restrictive food intake disorder: a case series of patients prescribed stimulant medication in a partial hospitalization program for eating disorders.” Journal of eating disorders vol. 11,1 226. 18 Dec. 2023, doi:10.1186/s40337-023-00954-1
Fu X, Wu W, Wu Y, Liu X, Liang W, Wu R, Li Y. Adult ADHD and comorbid anxiety and depressive disorders: a review of etiology and treatment. Front Psychiatry. 2025 Jun 6;16:1597559. doi: 10.3389/fpsyt.2025.1597559. PMID: 40547117; PMCID: PMC12179154.
Johnson, Simon et al. “Prevalence of attention deficit hyperactivity disorder/hyperkinetic disorder of pediatric and adult populations in clinical settings: a systematic review, meta-analysis and meta-regression.” Molecular psychiatry vol. 31,1 (2026): 576-586. doi:10.1038/s41380-025-03178-8
Kambanis, P Evelyna et al. “Prevalence and correlates of psychiatric comorbidities in children and adolescents with full and subthreshold avoidant/restrictive food intake disorder.” The International journal of eating disorders vol. 53,2 (2020): 256-265. doi:10.1002/eat.23191
Kaşak, Meryem et al. “Selective Eating and Sensory Sensitivity in Children With ADHD: A Comparative Study of ARFID Symptom Profiles.” The International journal of eating disorders vol. 58,10 (2025): 1991-2002. doi:10.1002/eat.24512
Kreider, Consuelo M et al. “Strategies for Coping with Time-Related and Productivity Challenges of Young People with Learning Disabilities and Attention-Deficit/Hyperactivity Disorder.” Children (Basel, Switzerland) vol. 6,2 28. 13 Feb. 2019, doi:10.3390/children6020028
Magnus, Warren, et al. “Attention Deficit Hyperactivity Disorder (ADHD).” PubMed, StatPearls Publishing, 8 Aug. 2023, www.ncbi.nlm.nih.gov/books/NBK441838/.
Menzel JE, Perry TR. Avoidant/Restrictive Food Intake Disorder: Review and Recent Advances. Focus (Am Psychiatr Publ). 2024 Jul;22(3):288-300. doi: 10.1176/appi.focus.20240008. Epub 2024 Jun 28. PMID: 38988468; PMCID: PMC11231462.
Nyholmer, Manda et al. “Neurodevelopmental and psychiatric conditions in 600 Swedish children with the avoidant/restrictive food intake disorder phenotype.” Journal of child psychology and psychiatry, and allied disciplines vol. 66,9 (2025): 1333-1344. doi:10.1111/jcpp.14134
Ramirez, Zerimar, and Sasidhar Gunturu. “Avoidant Restrictive Food Intake Disorder.” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK603710/.
Sader, Michelle et al. “The Co-Occurrence of Autism and Avoidant/Restrictive Food Intake Disorder (ARFID): A Prevalence-Based Meta-Analysis.” The International journal of eating disorders vol. 58,3 (2025): 473-488. doi:10.1002/eat.24369
Thomas, Jennifer J et al. “Cognitive-behavioral therapy for adults with avoidant/restrictive food intake disorder.” Journal of behavioral and cognitive therapy vol. 31,1 (2021): 47-55. doi:10.1016/j.jbct.2020.10.004
Watts, Rosie et al. “The clinical presentation of avoidant restrictive food intake disorder in children and adolescents is largely independent of sex, autism spectrum disorder and anxiety traits.” EClinicalMedicine vol. 63 102190. 30 Aug. 2023, doi:10.1016/j.eclinm.2023.102190









