Aversive ARFID: When Fear of Choking or Getting Sick Makes Eating Feel Unsafe


- Aversive ARFID is a type of avoidant/restrictive food intake disorder (ARFID) driven by fear of something going on while eating, not body image concerns.
- The fear is real and physical-feeling, often starting after a distressing food experience and reinforced over time through avoidance.
- With the right support—including exposure-based therapy—people can rebuild trust with food and feel safe eating again.

Most of us have had a bad experience with food at some point—choking, getting sick, or feeling suddenly nauseous. After something like that, it’s normal to be more cautious around food for a while, especially the specific food that made you feel bad. But for some people, that fear doesn’t fade, and can even develop into an eating disorder called aversive ARFID.
When this happens, foods that used to feel fine can start to feel risky. You might find yourself avoiding certain things—or eating less overall—because it just feels safer. Over time, that fear can take up more space and limit what feels possible to eat. This isn't just paranoia or overthinking; it’s a diagnosable condition.
Aversive ARFID is a form of avoidant/restrictive food intake disorder. It’s one of three main types of ARFID, alongside sensory sensitivity ARFID and lack of interest ARFID.
If you or a loved one feel fearful around food and are wondering whether it’s anxiety, a phobia, or something else entirely, you’re in the right place. Here, you’ll learn what aversive ARFID is, why it happens, and how treatment can help you or your loved one feel safe eating again.
What is aversive ARFID (fear of aversive consequences)?
Unlike many other eating disorders, ARFID isn’t about weight or body image. Instead, it’s driven by avoidance or restriction of food due to things like fear, sensory sensitivities, or a lack of interest in eating. And it can have a real impact on nutrition and overall health.
ARFID can affect people of any age and body size. It’s most commonly diagnosed in children—estimates suggest that anywhere from 0.3% to 15.5% of kids and teens may meet the criteria.
It can also continue into adulthood or even start later in life. While there’s less research on adults, current estimates suggest ARFID affects around 0.3% of the general adult population. Within that group, research suggests that aversive ARFID affects about one in three people.
Aversive ARFID is a type of ARFID where a person avoids food out of a fear that something bad will happen if they eat, like choking, having an allergic reaction, vomiting, or something else. You might hear this described as a “fear of aversive consequences,” but in plain terms, it just means being afraid of a negative physical reaction to food.
“People with fear of aversive consequences in ARFID think if they eat certain foods or a certain amount of food, something bad will happen after they eat,” says Michelle Jones, PhD, a licensed psychologist and clinical instructor at Equip. “They restrict the volume and/or variety of their food intake in an effort to prevent or reduce the perceived chance of a specific negative event occurring."
What fears are common in aversive ARFID?
At the center of aversive ARFID is fear. But it’s not just general anxiety—these fears tend to be very specific, physical, and tied to what might happen in the body during or after eating.
Common fears include:
- Choking or food getting stuck
- Vomiting or feeling nauseous
- Getting sick after eating
- Having an allergic reaction
- Stomach pain, gagging, or other uncomfortable sensations
In younger children, this can look a little different. Instead of clearly naming fears like choking or vomiting, they might say the food will taste bad, feel “disgusting,” or make them gag, according to Ilana Brodzki Pilato, PhD, a licensed clinical psychologist at Duke Center for Eating Disorders.
What are the signs and symptoms of aversive ARFID?
Aversive ARFID shows up in more than just food choices. It also shapes how eating feels, both physically and emotionally. The symptoms can look different from person to person, but they often revolve around trying to prevent a feared outcome. Here’s the breakdown.
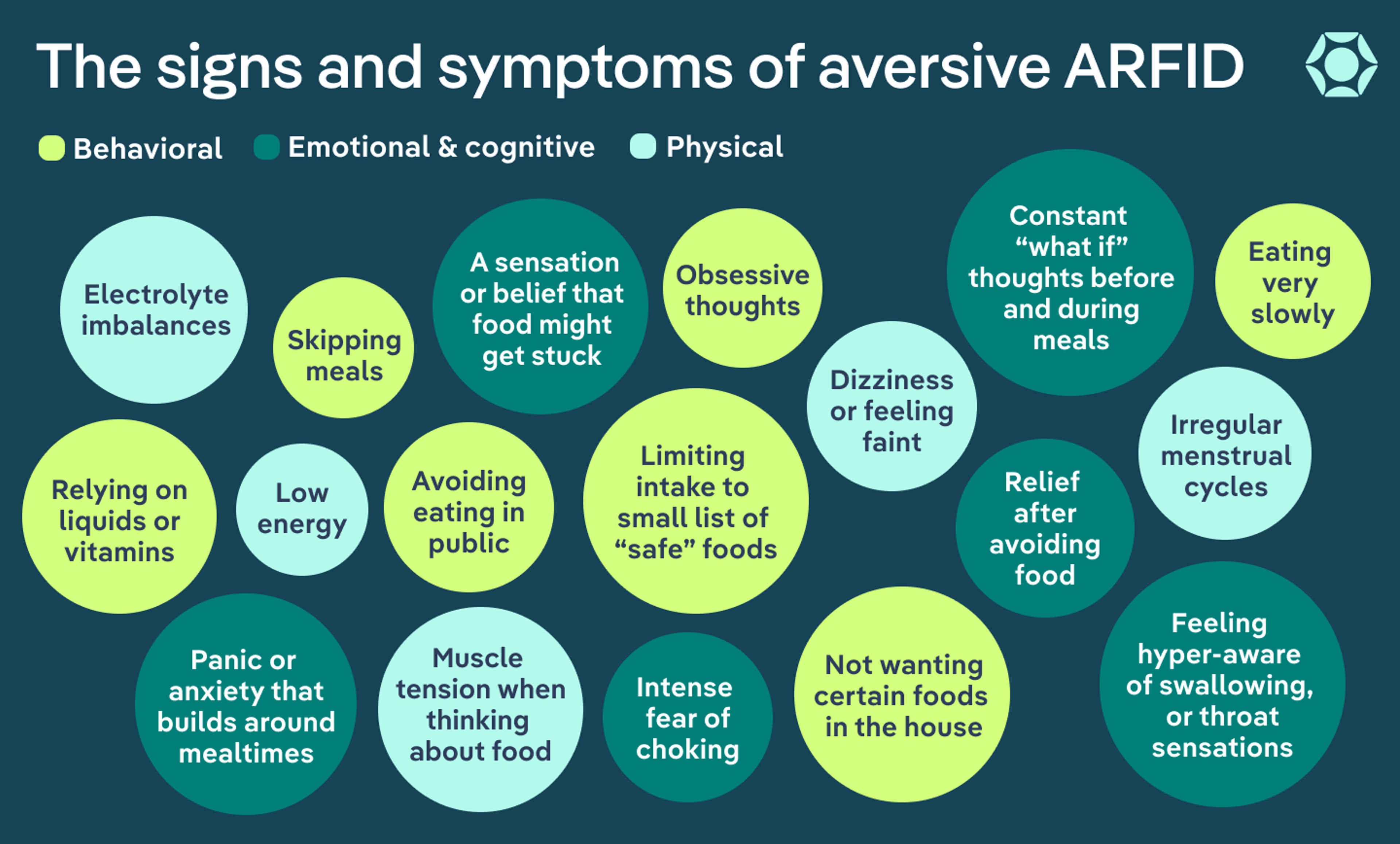
Behavioral signs
According to experts, aversive ARFID can affect how someone approaches food or meals. You might notice behaviors such as:
- Avoiding specific foods, entire food groups, or all solid foods because they feel unsafe
- Avoiding where the triggering event occurred
- Not wanting certain foods in the house
- Avoiding others eating certain foods
- Avoiding eating in front of others
- Obsessive thoughts and worries about food and food preparation
- Sticking to a very small list of “safe” foods
- Eating very slowly or taking unusually small bites
- Cutting food into tiny pieces or over-chewing to feel safer
- Skipping meals altogether, especially when anxiety is high
- Relying on liquids, supplements, or a feeding tube
Physical signs
Over time, eating less or limiting food variety can start to affect the body. According to Christine Ruberti-Bruning, MA, ATR-BC, CEDS, LPC, a certified eating disorder specialist at Ruberti Counseling Services, the restrictive eating associated with aversive ARFID can have a number of physical consequences, including:
- Unintended weight loss or difficulty maintaining weight
- For children, falling off their expected growth curve
- Nutritional deficiencies or malnutrition
- Electrolyte imbalances
- Low energy or fatigue
- Dizziness or feeling faint
- Gastrointestinal discomfort, especially as eating patterns change
- Constipation
- Irregular menstrual cycles
- Rapid heart rate, heavy breathing, and muscle tension when thinking about food
Emotional and cognitive signs
Much of the experience of aversive ARFID happens internally. A person struggling with this condition has thoughts and sensations that make eating feel stressful, unpredictable, and even dangerous rather than something routine or enjoyable.
Common thoughts and feelings include:
- Intense fear of choking, vomiting, or getting sick
- Constant “what if” thoughts before and during meals
- Feeling hyper-aware of swallowing, throat sensations, or stomach discomfort
- A sensation or belief that food might get stuck
- Panic or anxiety that builds around mealtimes
- Relief after avoiding food
How does aversive ARFID develop?
Aversive ARFID often starts with a shift in how your brain and body respond to food. For some people, this shift occurs after a specific experience, like choking, getting sick, or having an allergic reaction to food, says Ruberti-Bruning. The brain flags that moment as unsafe and starts trying to prevent it from happening again.
But that’s not always the case. For others, the fear builds more gradually over time. It might start with increased sensitivity to body sensations, ongoing anxiety, or a few uncomfortable experiences that slowly add up. And in some cases, it can seem to come out of nowhere without a clear trigger at all.
Because ARFID is a relatively new diagnosis (it was introduced into the DSM in 2013), researchers are still working to fully understand why it develops. What we do know is that, regardless of how it starts, the pattern that follows tends to look very similar.
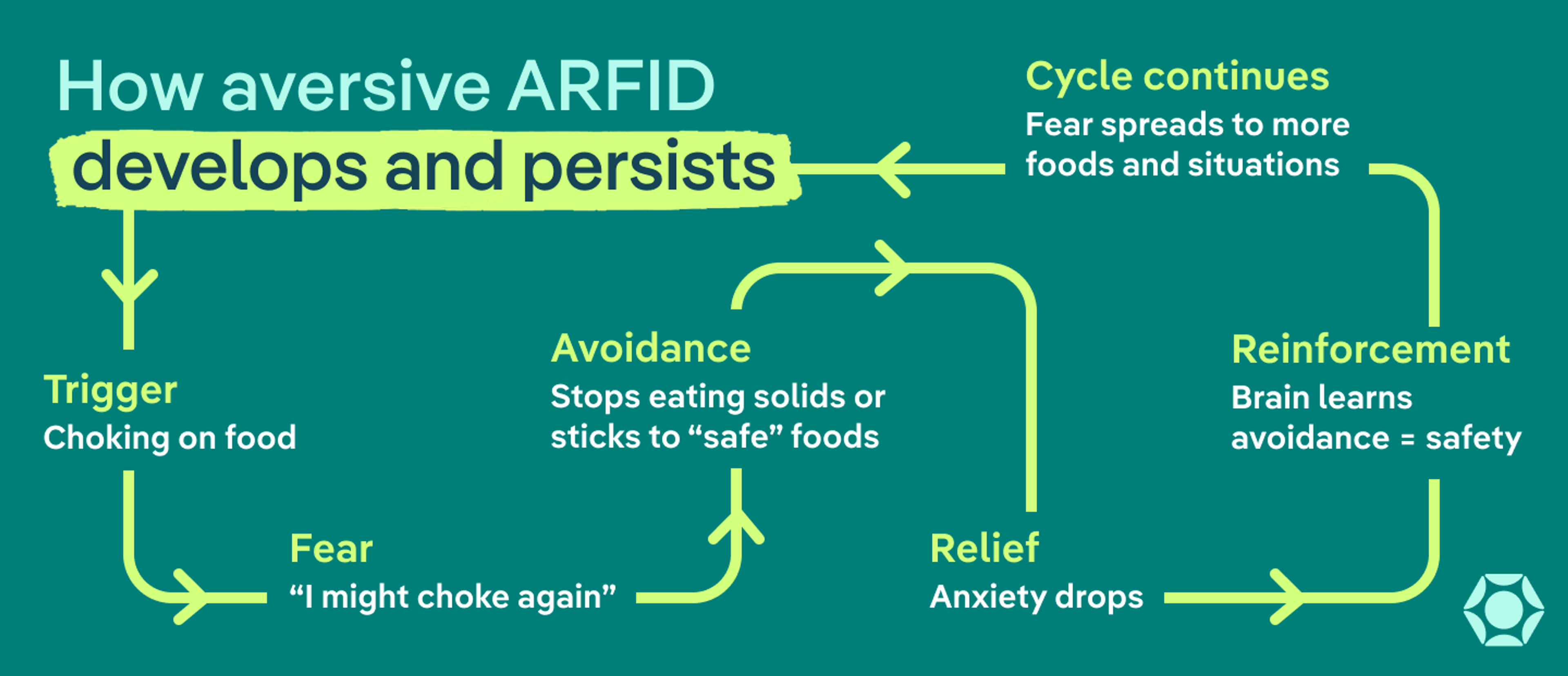
This pattern is often described as a fear-avoidance cycle:
- Trigger or shift: A distressing experience or gradual increase in fear around eating
- Fear: “What if something goes wrong?”
- Avoidance: Cutting out certain foods or eating situations
- Relief: Anxiety drops when you avoid the feared outcome
- Reinforcement: Your brain learns that avoidance = safety
The challenge is that this loop strengthens the fear of eating over time.
“When you're avoiding things, you're limiting your opportunities to challenge any inaccurate or unhelpful beliefs and thoughts around the likelihood of that traumatic event happening again. And you're underestimating your ability to tolerate any distress or discomfort from that,” says Jones. “You get stuck in a cycle of fear and avoidance that can be really difficult to break.”
That’s how something that began as a protective response can turn into a pattern that feels hard to break.
Are some people more vulnerable to aversive ARFID?
Not everyone who has a negative food experience develops ARFID. But some people may be more sensitive to this kind of response.
Factors that can increase vulnerability include:
- Heightened sensitivity to physical sensations (like throat or stomach discomfort)
- A tendency toward anxiety or strong fear responses
- Past experiences with choking, vomiting, food poisoning, or allergic reactions
- Medical conditions that affect swallowing or digestion
- A history of panic attacks, especially during or after eating
For people who have one or more of these risk factors, the body’s alarm system may activate more quickly and stay on high alert for longer, making it harder for the brain to recognize that eating is safe again.
Why these fears can feel so real
If you’re dealing with aversive ARFID, one of the most confusing parts is how physical it all feels.
Before eating, there’s often a sense of dread. While eating, you might notice every swallow, every sensation in your throat or stomach. Afterward, you might find yourself waiting to see if something goes wrong.
While this can be distressing, it’s also completely understandable. What’s actually happening is that your brain is trying to protect you—it’s just being a little overactive. Because of a heightened fear response, it starts treating normal sensations, like swallowing or digestion, as signs of danger. Over time, the fear can start to feel less like a possibility and more like a certainty.
From the outside, it might look like someone is just avoiding food. But on the inside, it feels like their body is telling them something isn’t safe—and they’re trying to listen.
That’s also why simply “pushing through” or forcing yourself (or someone else) to eat often backfires. When the body is in a threat state, pressure can actually increase fear, not reduce it.
The good news: This pattern can change. With the right support, your brain can relearn that eating is safe, and those physical and emotional symptoms can start to ease.
What are the long-term health risks of aversive ARFID?
When fear starts getting in the way of how much you can eat, your body can start to feel it. Even small shifts, over time, can add up. Some of the most common risks include:
- Nutritional deficiencies: Not getting enough variety can make it harder to meet basic nutrient needs, including vitamins and minerals your body relies on to function well.
- Low energy and fatigue: When your body isn’t getting enough fuel, it can lead to feeling tired, weak, or mentally foggy.
- Gastrointestinal issues: Eating less (or eating a very limited range of foods) can affect digestion, sometimes leading to discomfort, bloating, or slowed digestion.
- Weight loss or difficulty maintaining weight: For some people, intake becomes too limited to support their body’s needs.
- Delayed growth and development: Restriction during key growth periods can interfere with physical development in children and teens.
- Cardiovascular effects: In more severe cases, long-term malnutrition can affect heart rate, blood pressure, and overall cardiovascular health.
- Social and emotional impact: Meals can become stressful or isolating, which can affect relationships, routines, and overall quality of life.
Not everyone with aversive ARFID will experience all of these. But these risks highlight why this isn’t something to brush off as “just anxiety” or “just being careful.” The earlier aversive ARFID is recognized, the easier it is to step in and get support before any harmful effects become more serious.
If you’re unsure whether what you or a loved one are experiencing could be ARFID, taking a Equip’s clinically validated, ARFID-specific screener can be a helpful first step.
What’s the difference between aversive ARFID, anxiety, OCD, and phobias?
Aversive ARFID vs anxiety, OCD, and phobias
Condition | Core fear | Relationship to food | Nutritional effects |
Aversive ARFID | Something bad will happen when eating (like choking or getting sick) | Food itself feels unsafe, leading to avoidance | Often significant |
Anxiety | General worry or physical sensations (like nausea or a racing heart) | Eating may feel harder, but food isn’t always the main focus | Varies |
OCD | Intrusive thoughts and a need to prevent something bad from happening | Food may be part of rituals or avoidance patterns | Not always present |
Phobia | A specific object or experience (like choking or vomiting) | Food may or may not be involved | Usually limited |
All of these conditions can involve intense fear and avoidance. But with aversive ARFID, the fear is specifically tied to eating. It starts to affect how much or what someone can eat, to the point that it impacts physical and mental health.
With anxiety disorders, the fear is usually broader (like general worry or panic) and not limited to food. With OCD, it’s driven by intrusive thoughts and compulsions. And with specific phobias (like fear of choking or vomiting), the fear is more narrowly focused and doesn’t always lead to ongoing food restriction.
That said, they can absolutely overlap—and often do. What matters most is understanding the root cause and getting the right kind of support.
How is aversive ARFID treated?
Aversive ARFID treatment focuses on helping someone feel safe eating again.
“It requires a collaborative approach—a registered dietitian, a therapist, and a doctor or pediatrician are important members of the team,” says Ruberti-Bruning. “The level of care will be based on the medical impacts of ARFID.” Here are common components of treatment.
Medical and nutritional support / Weight restoration
If someone isn’t getting enough nutrition, the first priority is helping their body get what it needs. According to Pilato, that might mean:
- Increasing overall intake using “safe” foods
- Adding nutritional supplements
- Working toward weight restoration, if needed
For kids and teens, it’s usually less about hitting a specific weight and more about getting back on track with growth. And in more severe cases, higher levels of care—like inpatient or residential treatment—may be needed to help stabilize health, says Ruberti-Bruning.
Psychoeducation
“We pretty much always start off treatment by making sure the patient understands ARFID and how their experience with ARFID plays out,” says Jones. That includes looking at both past and current experiences: what triggered the fear, how it shows up now, and why the pattern sticks.
Patients also learn about the nutritional impact of ongoing restriction, which can help make the need for change feel more concrete. In addition, they’re educated about the treatment itself. Patients learn how exposure therapy works and why it’s effective, which helps build trust in the process.
“We’re asking them to basically face their worst fears on a regular basis,” Jones explains. “Sometimes, really understanding the rationale can help people shift their perspective.”
For younger children, this part of treatment may look different, says Ruberti-Bruning. In family-based treatment (FBT), caregivers take a more active role in helping their child eat, so the focus is less on the child fully understanding the process and more on supporting behavior change at home.
Graded exposure therapy

Exposure therapy is the core of treatment for aversive ARFID. Instead of avoiding the fear, the goal is to approach it slowly, safely, and with support.
Together with a therapist, patients build a “fear ladder” of foods, starting with what feels most manageable and gradually working up to what feels scariest (for example, going from looking at a feared food to eventually eating it).
From there, treatment focuses on working through that ladder step by step. In practice, graded exposure therapy usually involves:
- Starting with a low-stress food or situation
- Facing that fear in a small, manageable way (like looking at, touching, or tasting the food)
- Staying with the experience long enough for anxiety to rise and then come back down
- Repeating the step until it starts to feel easier
- Gradually moving up to more challenging foods or situations
“This helps the patient prove to themselves that those fears are unlikely to happen, and if they do, they can tolerate them better than they expect they might be able to,” Jones explains. “This supports new learning that counteracts the unhelpful beliefs that are holding them back from engaging in their lives, and it supports a gradual decrease in fear and anxiety over time.”
For younger patients, therapists may teach kids about their body sensations in a more playful way rather than using a formal fear hierarchy. They might use fun characters or stories to do this. Pilato says the goal is to help children feel curious about those sensations, rather than afraid.
What does recovery look like?
For many people, recovery from aversive ARFID starts with small shifts. Eating might feel a little less overwhelming. The “what if” thoughts may still be there, but they feel quieter or easier to move through.
Over time, those changes can build. You might notice:
- More foods start to feel safe
- Less fear around choking, vomiting, or getting sick
- Eating becomes more automatic again, instead of something you have to think through
- Less mental energy spent worrying before, during, or after meals
That doesn’t mean the fear disappears completely—there may still be moments where it shows up, and that’s okay. But what’s important is that it feels manageable and doesn’t control food choices or life in the same way.
Setbacks can also be part of the process. A difficult experience or stressful period can temporarily bring back the fear. It’s important to remember that this is a normal part of recovery, and doesn’t mean you’re back at square one. With the right support, it’s possible to keep moving forward.
When to seek help
You don’t have to wait until things feel severe. If eating feels hard or limiting for you or a loved one, that’s reason enough to get support.
According to Jones, other signs it may be time to get help include:
- Avoiding more and more foods or meals
- Eating feels stressful, scary, or exhausting
- Weight loss, low energy, or other physical changes
- Relying on a very small list of “safe” foods
- Avoiding social situations that involve food
Working with a provider who understands ARFID can help you (or your loved one) feel safer around food and start to rebuild flexibility over time. Note that not all providers—even those who specialize in eating disorders—are knowledgeable about ARFID. But true experts are available, and it’s important to seek out an ARFID-informed provider for the best care.
The bottom line
If eating has started to feel stressful, unpredictable, or even unsafe, you’re not imagining it, and you’re not alone. Aversive ARFID is a real, recognized eating disorder driven by fear, not choice. And while that fear can feel overwhelming (and very physical), it’s also something that can change with the right support.
With treatment, it’s possible to rebuild trust with food, expand what feels safe to eat, and spend less time and energy worrying about meals.
Frequently asked questions (FAQs)
Can fear of choking lead to an eating disorder?
Yes, fear of choking can sometimes turn into avoidant/restrictive food intake disorder (ARFID), specifically the fear-based type.
If you’ve choked before—or even just feel like you might—it can start to change how you eat. You might avoid certain foods, take smaller bites, or stick to whatever feels safest. And over time, that fear can grow and start to limit what and how much you’re able to eat.
What does it mean if someone is afraid to eat?
It can mean different things, but in some cases, it’s a sign of ARFID—especially if the fear of food is tied to something bad happening, like choking, vomiting, or getting sick.
When that fear starts to affect how much someone eats, what foods feel safe, or their overall health, it’s worth looking into further.
Is aversive ARFID the same as anxiety?
Not exactly. Aversive ARFID and anxiety can look similar—and often overlap—but ARFID is specifically centered around eating. The fear directly affects food intake and can lead to nutritional or health impacts, which is what makes it an eating disorder.
Brigham, Kathryn S et al. “Evaluation and Treatment of Avoidant/Restrictive Food Intake Disorder (ARFID) in Adolescents.” Current pediatrics reports vol. 6,2 (2018): 107-113. doi:10.1007/s40124-018-0162-y
Brock, Hannah, et al. “Obsessive-Compulsive Disorder (OCD).” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK553162/.
Burton-Murray, Helen et al. “Medical Comorbidities, Nutritional Markers, and Cardiovascular Risk Markers in Youth With ARFID.” The International journal of eating disorders vol. 57,11 (2024): 2167-2175. doi:10.1002/eat.24243
Christian, Caroline et al. “Development and Validation of a Broad and Fear-Adaptable Measure of Fear Approach and Application to Common Eating Disorder Fears.” Assessment vol. 31,3 (2024): 602-616. doi:10.1177/10731911231174469
D'Adamo, Laura et al. “Prevalence, Characteristics, and Correlates of Avoidant/Restrictive Food Intake Disorder among Adult Respondents to the National Eating Disorders Association Online Screen: A Cross-Sectional Study.” Research square rs.3.rs-3007049. 5 Jun. 2023, doi:10.21203/rs.3.rs-3007049/v1. Preprint.
Di Luzio, Michelangelo et al. “Understanding the Relationship Between Avoidant/Restrictive Food Intake Disorder and Obsessive-Compulsive Symptoms: A Systematic Review.” Nutrients vol. 18,5 874. 9 Mar. 2026, doi:10.3390/nu18050874
Eddy, Kamryn. “Avoidant Restrictive Food Intake Disorder - NEDA.” National Eating Disorders Association, 11 June 2024, www.nationaleatingdisorders.org/avoidant-restrictive-food-intake-disorder-arfid/.
Fonseca, Natasha K O et al. “Avoidant restrictive food intake disorder: recent advances in neurobiology and treatment.” Journal of eating disorders vol. 12,1 74. 7 Jun. 2024, doi:10.1186/s40337-024-01021-z
George, Steven Z et al. “Comparison of graded exercise and graded exposure clinical outcomes for patients with chronic low back pain.” The Journal of orthopaedic and sports physical therapy vol. 40,11 (2010): 694-704. doi:10.2519/jospt.2010.3396
Gianneschi, Julia R et al. “Assessing Fears of Negative Consequences in Children With Symptoms of Avoidant Restrictive Food Intake Disorder.” The International journal of eating disorders vol. 57,12 (2024): 2329-2340. doi:10.1002/eat.24303
Menzel, Jessie E, and Taylor R Perry. “Avoidant/Restrictive Food Intake Disorder: Review and Recent Advances.” Focus (American Psychiatric Publishing) vol. 22,3 (2024): 288-300. doi:10.1176/appi.focus.20240008
Penninx, Brenda Wjh et al. “Anxiety disorders.” Lancet (London, England) vol. 397,10277 (2021): 914-927. doi:10.1016/S0140-6736(21)00359-7
Ramirez, Zerimar, and Sasidhar Gunturu. “Avoidant Restrictive Food Intake Disorder.” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK603710/.
Samra, Chandan K, and Sara Abdijadid. “Specific Phobia.” Nih.gov, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK499923/.
Seetharaman, Sujatha, and Errol L Fields. “Avoidant/Restrictive Food Intake Disorder.” Pediatrics in review vol. 41,12 (2020): 613-622. doi:10.1542/pir.2019-0133
Stern, Casey M et al. “Difficulties in Emotion Regulation in Avoidant/Restrictive Food Intake Disorder.” The International journal of eating disorders vol. 57,11 (2024): 2156-2166. doi:10.1002/eat.24281
Thomas, Jennifer J et al. “Avoidant/Restrictive Food Intake Disorder: a Three-Dimensional Model of Neurobiology with Implications for Etiology and Treatment.” Current psychiatry reports vol. 19,8 (2017): 54. doi:10.1007/s11920-017-0795-5
Thomas, Jennifer J et al. “Cognitive-behavioral treatment of avoidant/restrictive food intake disorder.” Current opinion in psychiatry vol. 31,6 (2018): 425-430. doi:10.1097/YCO.0000000000000454
Thomas, Jennifer J et al. “Neural Response to Food Cues in Avoidant/Restrictive Food Intake Disorder.” JAMA network open vol. 8,2 e2460101. 3 Feb. 2025, doi:10.1001/jamanetworkopen.2024.60101
Thomas, Jennifer J, and Kamryn T Eddy. “Cognitive-Behavioral Model of ARFID.” Cambridge University Press EBooks, 26 Oct. 2018, pp. 20–25, www.cambridge.org/core/books/abs/cognitivebehavioral-therapy-for-avoidantrestrictive-food-intake-disorder/cognitivebehavioral-model-of-arfid/447D7644CC0AC85E5996CD1F7FDC281A, https://doi.org/10.1017/9781108233170.006.
Zucker, Nancy L et al. “Feeling and body investigators (FBI): ARFID division-An acceptance-based interoceptive exposure treatment for children with ARFID.” The International journal of eating disorders vol. 52,4 (2019): 466-472. doi:10.1002/eat.22996









