Understanding ARFID Symptoms in Children, Teens, and Adults


- ARFID is more than picky eating. It can affect nutritional status, physical and mental health, relationships, school, work, and everyday life.
- The signs of ARFID aren't always obvious. Many people spend years wondering whether they're dealing with anxiety, digestive issues, sensory differences, or something else.
- ARFID can look different from person to person. Some people avoid food due to sensory sensitivities, some fear negative experiences while eating, and others have little interest in food.
- ARFID can affect people of all ages. While it often begins in childhood, teens and adults can experience ARFID too.
- If eating challenges are causing distress or making daily life harder, support is available, and recovery is possible with the right treatment.

At first glance, avoidant/restrictive food intake disorder (ARFID) can look like picky eating. But ARFID is a serious eating disorder that goes much deeper than food preferences. Unlike other eating disorders, ARFID isn't driven by body image concerns or a desire to lose weight. Instead, food avoidance and other ARFID symptoms are typically linked to sensory sensitivities, fear around eating, or a lack of interest in food (or a combination of these factors).
"My ARFID is driven by a fear of vomiting, or emetophobia, due to having a history of chronic nausea and health issues as well as significant anxiety," says Equip Peer Mentor Kelsey Gilchriest, who has experienced ARFID firsthand.
Her story highlights an important reality: ARFID manifests in complex and unique ways, and doesn't always look the way people expect it to. And because symptoms vary from person to person, it’s often mistaken for picky eating, anxiety, digestive issues, or something else entirely.
Below, we'll cover the most common signs of ARFID, how symptoms can present across ages and life stages, and when it may be time to seek support.
What are the symptoms of ARFID?
ARFID symptoms affect more than eating habits alone. It can also impact physical health, emotional well-being, nutritional status, and social functioning.
While every person's experience is unique, ARFID symptoms generally fall into three broad presentations: sensory-based ARFID, fear-based ARFID, and low-interest ARFID. Some people fit clearly into one category, while others experience a combination of symptoms from multiple presentations.
Here’s a breakdown of the different behavioral, emotional, physical, and social signs that occur across each type of ARFID.
ARFID Symptoms at a Glance
Behavioral | Emotional | Physical/Nutritional | Social | |
Common across many people with ARFID | Limited food variety; avoidance of certain foods or food groups; eating habits interfere with daily life | Distress around eating; frustration; embarrassment; shame | Nutritional deficiencies; fatigue; difficulty meeting energy needs; growth concerns in children and teens | Meals become stressful; eating challenges affect school, work, relationships, or family life |
Sensory-based ARFID | Avoids certain textures, tastes, smells, temperatures, or appearances; may only eat specific brands or preparations | Discomfort, distress, or disgust when exposed to non-safe foods | Limited food variety may make it harder to meet nutritional needs | Avoids restaurants, parties, or other situations where preferred foods may not be available |
Fear-based ARFID | Avoids foods associated with choking, vomiting, allergic reactions, stomach pain, or other feared outcomes | High anxiety around eating; persistent food-related fears | Reduced intake can lead to weight loss, nutritional deficiencies, or low energy | Avoids unfamiliar foods, restaurants, or social situations involving food |
Lack-of-interest ARFID | Forgets to eat; skips meals; loses interest after a few bites; eats very small portions | Little interest in food or eating; eating may feel like a chore | Low energy intake, poor growth, weight loss, fatigue, or nutritional deficiencies | May avoid meal-related activities because eating feels burdensome or unimportant |
Behavioral signs
The behavioral signs of ARFID often center around avoiding, limiting, or struggling with food in ways that go beyond typical food preferences.
"What this [can] look like in practice is a kiddo who is beyond what parents might consider typical 'picky eating,' or a young adult or adult who eats a very limited range of foods, often foods that might be associated with younger ages," says Cait Scafati, MA, MSW, LCSW, virtual mental health clinical director at Clear Behavioral Health.
While not everyone experiences the same symptoms, common behavioral signs include:
- Eating a very limited range of foods: Some people with ARFID feel comfortable eating only a small number of "safe" foods or avoid certain food groups altogether. “Oftentimes, it’s easier to ask what a client will eat rather than what they won’t,” says Scafati.
- Avoiding foods based on sensory characteristics: Certain textures, smells, tastes, temperatures, colors, or appearances may make foods feel intolerable.
- Needing foods prepared in a specific way: Small changes to a recipe, brand, packaging, or preparation method may make a food feel impossible to eat.
- Eating very small portions: Some people become full quickly, have little interest in food, or struggle to eat enough throughout the day.
- Taking a long time to eat: Meals may feel overwhelming, stressful, or physically difficult to complete.
- Avoiding eating after a negative experience: Food poisoning, an allergic reaction, or another traumatic food-related event may lead someone to restrict foods they perceive as unsafe, or food generally.
- Continuing to avoid food despite hunger: ARFID is not simply a matter of refusing food until hunger wins out. “Clients will not eat despite significant hunger," says Scafati.
- Relying on nutritional supplements or meal replacement drinks: Some people use supplements to help meet nutritional needs when eating enough food feels difficult.
Emotional signs
ARFID can also affect how someone feels about eating. According to Scafati and Equip therapist Carol Brown, MSW, common emotional signs include:
- Anxiety around food or eating: Some people feel intense worry before meals, especially when they aren't sure whether preferred foods will be available.
- Fear of negative consequences: People with fear-based ARFID may worry about unpleasant or dangerous outcomes.
- Distress when routines change: Unexpected changes to meals, restaurants, brands, or food preparation can feel upsetting.
- Feeling overwhelmed by certain foods: Foods with unfamiliar textures, smells, tastes, or appearances may trigger strong feelings of discomfort or disgust.
- Little interest in food or eating: Some people rarely feel hungry, forget to eat, or view eating as a chore rather than something enjoyable.
- Frustration around eating challenges: Many people recognize that their eating habits are limiting, but feel unable to change them on their own.
- Shame or embarrassment about food preferences: Older children, teens, and adults may feel self-conscious about eating differently from their peers.
- Feeling misunderstood by others: ARFID is often dismissed as "just picky eating," which can leave people feeling judged or isolated.
- Stress around mealtimes: Meals may become a source of tension, conflict, or worry for both the person with ARFID and their family. Brown notes that for younger kids with ARFID, “ the emotional impact is often felt most by their caregivers who work hard to mitigate the impact of ARFID.”
Physical signs
ARFID can make it difficult to get adequate nutrition, which can affect physical health. According to the experts, physical signs of ARFID can include:
- Weight loss or difficulty gaining weight as expected: This may be especially noticeable in children and teens who are still growing. That said, it’s important to remember that someone can have ARFID—and be struggling significantly—without losing weight.
- Delayed growth or development: Similarly, inadequate nutrition may affect normal growth and development in kids and teens.
- Nutritional deficiencies: Restricting certain foods or food groups can make it harder to get enough vitamins, minerals, and other nutrients.
- Low energy levels: Not getting enough nutrition can leave people feeling fatigued.
- Dizziness or lightheadedness: Inadequate nutrition can affect energy levels, blood sugar regulation, and overall physical functioning.
- Feeling cold frequently: The body may have difficulty maintaining temperature when it isn't getting enough energy.
- Gastrointestinal issues: Stomach pain, constipation, nausea, or other digestive symptoms may occur alongside ARFID. In some cases, these symptoms can both contribute to and result from restrictive eating.
- Difficulty concentrating: The brain needs adequate nutrition to function optimally, so it's harder to focus when those needs aren't met.
- Changes in hair, skin, or nails: Nutritional deficiencies can sometimes show up as brittle nails, hair thinning, dry skin, or other physical changes.
Social signs
For many people, some of the most noticeable effects of ARFID happen outside the kitchen, impacting their social functioning and relationships with others, says Scafati. The social signs of ARFID can include:
- Avoiding social events that involve food: Parties, school events, dates, or work functions may feel stressful when preferred foods aren't available.
- Spending significant time planning around food: Some people check menus in advance, bring their own food, or avoid situations where safe foods may be hard to find.
- Feeling isolated or left out: Repeatedly declining invitations or having different eating habits than peers can make it harder to feel included and connected.
- Embarrassment or self-consciousness around eating: Some people worry about being judged for their eating habits.
- Family life revolving around food concerns: Parents and caregivers may spend considerable time negotiating meals, accommodating food restrictions, or avoiding certain activities or events because of eating challenges.
- Difficulties at school or work: Eating challenges may interfere with field trips, sleepovers, business meetings, workplace lunches, travel, or other activities involving food.
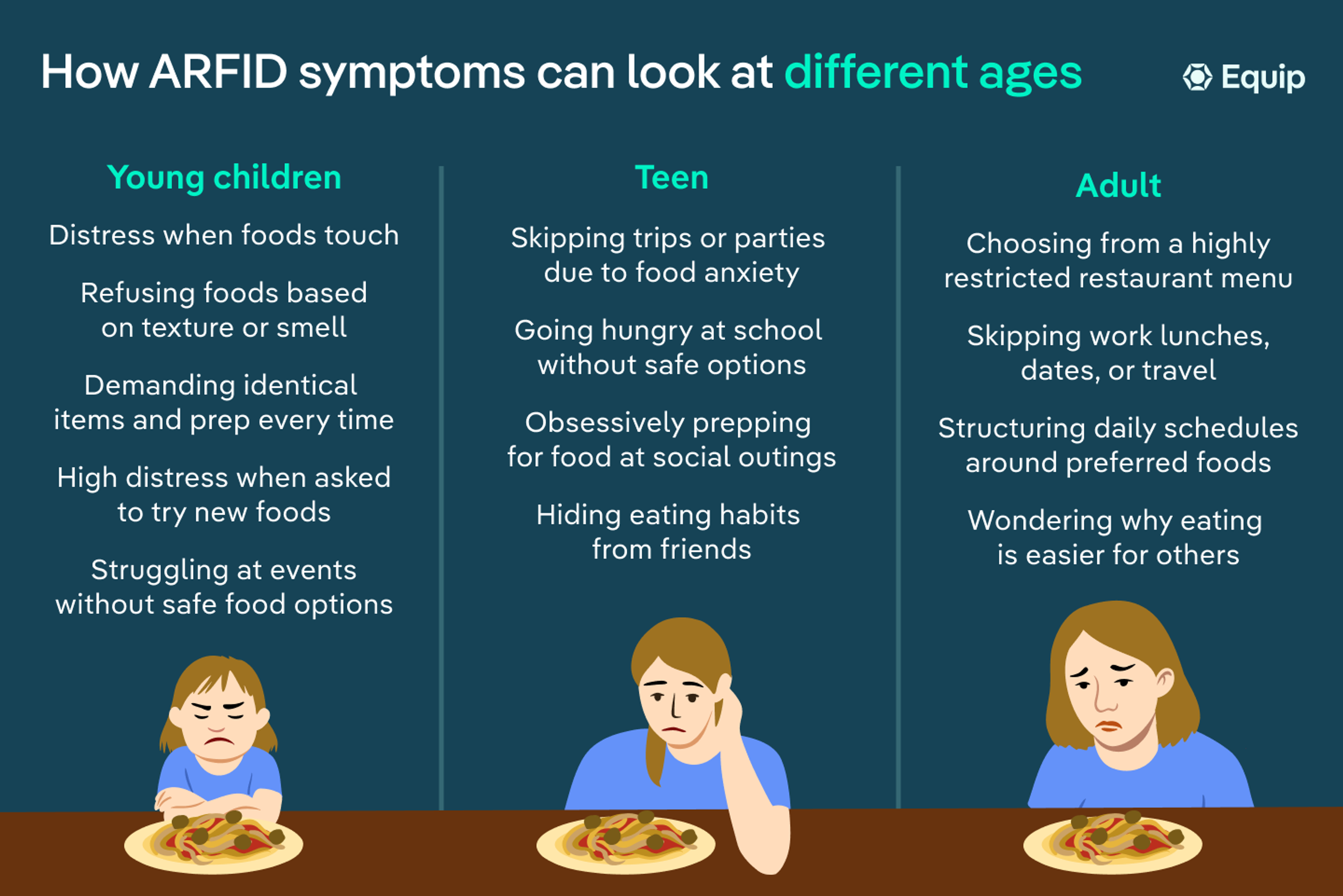
How ARFID can look different in kids, teens, and adults
“Although the DSM criteria for ARFID is the same no matter what the age group, ARFID presentation differs in kids, teens, and adults,” says Brown. Here’s how.
Young children | Teens | Adults |
|
|
|
ARFID symptoms in young children
First things first, if you’re concerned a young child in your life may have ARFID, it’s important to note that ARFID is different from pediatric feeding disorder (PFD), although the two conditions can sometimes overlap. PFD involves feeding challenges caused by medical, developmental, or oral-motor difficulties. ARFID, on the other hand, is a mental health condition in which food restriction affects nutrition, growth, or daily functioning.
ARFID in kids is often noticeable during everyday moments like family meals, school lunches, birthday parties, or trips to the grocery store. According to Brown, parents may notice their child:
- Eats only a small number of foods and strongly resists trying new ones
- Refuses foods based on their texture, smell, color, temperature, or appearance
- Becomes upset when foods touch each other or aren't prepared in a specific way
- Insists on certain brands, packaging, or presentation of foods
- Experiences significant distress around unfamiliar foods
- Struggles at playdates, birthday parties, or other activities where preferred foods aren't available
- Has difficulty gaining weight, growing as expected, or meeting nutritional needs
ARFID symptoms in teens
As children get older, ARFID can become less visible—but no less challenging.
Teens are often more aware of how their eating habits compare to those of their peers, and many become skilled at hiding their struggles. “The emotional impact increases with age and independence,” explains Brown.
In practice, she says a teen with ARFID might:
- Eat the same small group of "safe" foods day after day
- Skip school lunches because they don't feel comfortable with the available options
- Feel anxious about eating at restaurants, friends' houses, or social gatherings
- Avoid activities like sleepovers, camps, or team events where food is less predictable
- Feel embarrassed or self-conscious about their eating habits
- Spend significant time planning ahead to make sure safe foods will be available
- Experience low energy, difficulty concentrating, or other effects of inadequate nutrition
ARFID symptoms in adults
Although ARFID often begins in childhood, many people aren't diagnosed until adulthood. By then, many have developed routines that help them navigate around their symptoms. As a result, symptoms of ARFID in adults may not be obvious—even when eating still takes significant mental energy and planning.
According to Brown, adults with ARFID might:
- Rely on the same handful of foods they've eaten for years
- Rely heavily on takeout
- Order from a limited menu when dining out
- Avoid social events or travel that involve unfamiliar foods
- Spend significant time planning meals around safe foods
- Feel embarrassed about eating differently
- Experience ongoing nutritional deficiencies or other health concerns related to restrictive eating
- Realize that food takes up more mental space than it seems to for other people
- Experience financial burdens due to ARFID-related food waste
How autism, ADHD, and other conditions can shape ARFID symptoms
ARFID can affect anyone. But “neurodivergence and ARFID have high levels of overlap, and can also make recovery more complex when individuals are experiencing both simultaneously,” says Brown.
Indeed, research shows ARFID is more common among people with certain conditions, including autism, ADHD, anxiety disorders, and obsessive-compulsive disorder (OCD).
These conditions don't necessarily cause ARFID, but they can influence how symptoms show up. For example:
- Someone with ARFID and autism may experience intense sensory sensitivities that make certain textures, smells, or flavors difficult to tolerate.
- Someone with anxiety may be more likely to develop fears around food.
- Someone with ARFID and ADHD may struggle to notice hunger cues, forget to eat, or find meal planning challenging.
- Someone with ARFID and OCD may avoid certain foods because of contamination fears.
At the same time, not everyone with ARFID is neurodivergent, and not every neurodivergent person develops ARFID, says Scafati. Understanding what's driving the food avoidance—and any underlying conditions that may be shaping it—can help point the way toward effective ARFID treatment.
Why ARFID symptoms are often misunderstood
If you've recognized yourself or your child in some of the examples throughout this article, you may be wondering why you didn’t consider ARFID sooner.
That’s common, and it’s not your fault. The truth is, ARFID often flies under the radar because it doesn't look like what many people think an eating disorder “should” look like. But that doesn’t make your challenges any less real or deserving of support.
According to both experts, ARFID is commonly overlooked for a variety of reasons, including:
- It's mistaken for picky eating: ARFID goes beyond food preferences. According to Scafati, people with ARFID may continue avoiding foods despite significant hunger, and the eating challenges often affect nutrition, health, or daily life.
- It's attributed to anxiety alone: Fear of negative experiences with food is a common ARFID presentation that’s easy to mistake for anxiety by itself.
- It's confused with digestive issues: Symptoms like nausea, stomach pain, or constipation can overlap with ARFID, sometimes making the eating disorder harder to recognize.
- It's explained away as sensory differences: Sensory sensitivities are common in people with autism and ADHD. But when food avoidance begins affecting nutrition or daily functioning, ARFID may also be part of the picture.
- It's overlooked in adults: Many adults have spent years adapting to their symptoms, making their struggles less obvious to others (and sometimes even to themselves).
When to seek help—and what treatment looks like
If these symptoms sound familiar and you think you or a loved one may be struggling with ARFID, it’s worth getting an evaluation. There’s no benchmark for being “sick enough” to deserve care, and when left untreated, ARFID can lead to serious physical and mental health complications, and interfere with relationships and everyday life. Talking to a trusted doctor or seeking an ARFID-informed eating disorder specialist is the first step toward getting the care you or your loved one deserve.
Treatment typically begins with a comprehensive evaluation to better understand a person's eating patterns, nutritional needs, medical history, and the factors contributing to food avoidance. Care should always involve a multidisciplinary team of AFID-informed individuals, including a therapist and dietitian, and often a physician if nutritional deficiencies or other health complications are present.
From there, treatment often focuses on helping people expand their range of foods, improve nutritional intake, reduce fear and anxiety around eating, and build confidence during meals, she adds. For children and teens, caregivers also play an important role in the recovery process. Depending on a person’s needs, treatment may include evidence-based approaches like:
- Cognitive behavioral therapy for ARFID (CBT-AR): A type of therapy that helps people gradually expand their range of foods and address unhelpful thoughts or fears around eating.
- Family-based treatment for ARFID (FBT-ARFID): This is an ARFID-specific variation of family-based treatment (FBT), which is the gold standard for treating eating disorders in young people. It empowers caregivers to support nutritional rehabilitation and recovery.
- Exposure and response prevention (ERP): This type of therapy helps people gradually face feared foods, eating situations, or sensory experiences.
No matter your situation, know that ARFID is treatable, and recovery is possible. If you're concerned about yourself or a loved one, our clinically validated ARFID screener is a good place to start. You can also schedule a consultation with Equip—the largest ARFID treatment provider in the U.S.—to explore treatment.
The bottom line
ARFID is a serious eating disorder that can affect nutrition, physical health, emotional well-being, and daily life. Because symptoms can look different from person to person, ARFID is often overlooked or mistaken for anxiety, digestive issues, or picky eating.
If you recognize symptoms of ARFID in yourself or a loved one, it's worth paying attention to them. ARFID is a real and treatable condition, and with the right support, you can build a healthier relationship with food and feel less limited by eating challenges.
Frequently asked questions (FAQs)
What does ARFID feel like?
The experience varies by person. Some people feel intense discomfort around certain textures, tastes, or smells. Others experience fear related to eating. Some simply have very little interest in food or eating. Many people with ARFID describe meals as stressful, exhausting, or something that requires far more planning and mental energy than it does for other people.
Can ARFID develop suddenly?
Sometimes. ARFID can develop after a distressing experience involving food, such as choking, food poisoning, or an allergic reaction. In other cases, symptoms emerge gradually over time, often beginning in childhood. Some people aren't diagnosed until years later, even though they've experienced symptoms for much of their lives.
Does ARFID last into adulthood?
Yes. While ARFID often begins in childhood, many people continue experiencing symptoms as teens or adults. Some adults don't realize their eating challenges may be related to an eating disorder until they learn more about ARFID later in life. The good news is that support is available at any age, and it's never too late to seek help.
1. Dinkler, Lisa et al. “Etiology of the Broad Avoidant Restrictive Food Intake Disorder Phenotype in Swedish Twins Aged 6 to 12 Years.” JAMA psychiatry vol. 80,3 (2023): 260-269. doi:10.1001/jamapsychiatry.2022.4612
2. Sharp, William G et al. “Feeding problems and nutrient intake in children with autism spectrum disorders: a meta-analysis and comprehensive review of the literature.” Journal of autism and developmental disorders vol. 43,9 (2013): 2159-73. doi:10.1007/s10803-013-1771-5
3. Kozak, Agata et al. “Avoidant/Restrictive Food Disorder (ARFID), Food Neophobia, Other Eating-Related Behaviours and Feeding Practices among Children with Autism Spectrum Disorder and in Non-Clinical Sample: A Preliminary Study.” International journal of environmental research and public health vol. 20,10 5822. 14 May. 2023, doi:10.3390/ijerph20105822
4. Seetharaman, Sujatha, and Errol L Fields. “Avoidant/Restrictive Food Intake Disorder.” Pediatrics in review vol. 41,12 (2020): 613-622. doi:10.1542/pir.2019-0133
5. Substance Abuse and Mental Health Services Administration. DSM-5 Changes: Implications for Child Serious Emotional Disturbance [Internet]. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2016 Jun. Table 22, DSM-IV to DSM-5 Avoidant/Restrictive Food Intake Disorder Comparison. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519712/table/ch3.t18/
6. Archibald, Tanith, and Rachel Bryant-Waugh. “Current evidence for avoidant restrictive food intake disorder: Implications for clinical practice and future directions.” JCPP advances vol. 3,2 e12160. 3 Apr. 2023, doi:10.1002/jcv2.12160
7. Zucker, Nancy et al. “Psychological and Psychosocial Impairment in Preschoolers With Selective Eating.” Pediatrics vol. 136,3 (2015): e582-90. doi:10.1542/peds.2014-2386









