ARFID vs. Picky Eating: Understanding the Difference


- Picky eating is common in early childhood and often improves with time, patience, and gentle exposure to new foods.
- ARFID is not a developmental phase, but a diagnosable eating disorder. It differs from picky eating because it significantly affects health, growth, nutrition, and/or daily life. It also typically becomes more restrictive over time and can lead to reliance on supplements and/or major distress and avoidance around meals.
- The food restriction associated with ARFID isn’t about body image or a desire to lose weight. It’s usually driven by sensory sensitivity, fear (like choking or vomiting), and/or a low interest in eating.
- You don’t have to wait until things feel “serious enough” to ask for help. Early, ARFID-informed treatment can protect health, and ease stress for the whole family.

Picky eating is common, especially in toddlers and young kids. Most of the time, that’s developmentally typical. But sometimes, what looks like extreme picky eating is actually avoidant/restrictive food intake disorder (ARFID)—an eating disorder that goes beyond preferences and begins to affect health, growth, nutrition, and daily life. But where’s the line between ARFID vs. picky eating?
“ARFID is often misunderstood as ‘just picky eating,’” says Christine Ruberti-Bruning, LPC, a certified eating disorder specialist at Ruberti Counseling Services. “The major difference is ARFID behaviors are highly disruptive to someone's quality of life and can have significant impacts on physical health.”
Maybe dinner turns into a standoff, or maybe your child’s list of “safe” foods keeps shrinking to the point that they’re not growing normally. If you’re an adult, you might be realizing that your limited range of foods isn’t just a quirky preference—it’s something that’s quietly shaped your life for years.
Below, we’ll walk through the difference between ARFID and picky eating, the warning signs to look for, and how to find ARFID-informed care that helps you (or you child) find lasting recovery.
What is picky eating?
Picky eating is a common part of childhood development, especially between the toddler and early elementary years (that’s about two to six years old). It can be frustrating for parents, but it’s usually driven by typical developmental factors, like a growing desire for independence or a heightened sensitivity to taste and texture that softens over time.
According to Michelle Jones, PhD, a licensed clinical psychologist and clinical instructor at Equip, signs of typical picky eating may include:
- Preferring familiar foods over new ones
- Avoiding certain textures or flavors but tolerating others
- Eating from most food groups, even if options are limited
- Gradually expanding foods with low-pressure exposure
- Continuing to grow along their expected height and weight curve
- Participating in social meals, even if they eat selectively
Importantly, picky eating doesn’t usually interfere with a child’s overall growth, health, or day-to-day life, she adds. In other words, food preferences can be strong, but they’re not shrinking someone’s world.
Picky eating can absolutely test your patience. But in most cases, it peaks in the toddler years and slowly improves as children gain exposure, confidence, and maturity.
What is avoidant/restrictive food intake disorder (ARFID)?
ARFID is an eating disorder, but not the kind most people picture.
Unlike anorexia or bulimia, ARFID isn’t driven by body image concerns or a desire to lose weight (although people with ARFID can still experience body image concerns, just like anyone else). Instead, it’s typically fueled by things like sensory sensitivities (for example, intense food texture aversion), fear of something bad happening while eating (like choking or vomiting), or a low interest in food altogether.
Over time, this pattern of restrictive eating can mean someone isn’t getting enough food variety or volume to meet their body’s needs. And that’s where one key difference between ARFID and picky eating becomes clear: ARFID leads to meaningful impacts on health, nutrition, growth, or daily life.
According to the DSM-IV-TR criteria, a person can be diagnosed with ARFID if their eating disturbance leads to at least one of the following:
- Significant weight loss (or failure to gain expected weight in children)
- Nutritional deficiencies
- Dependence on nutritional supplements or tube feeding
- Eating interfering with daily life (for example, avoiding school, social events, restaurants, or travel because of food).
ARFID in children can show up earlier than many people expect. According to Ruberti-Bruning, children can develop ARFID as early as four years old, though it tends to be more commonly diagnosed between 10 and 12 years old. Early symptoms of ARFID may include:
- A lack of interest in food
- Low appetite
- Eating only a very limited number of foods
- Needing foods prepared in highly specific ways
And although ARFID is more commonly diagnosed in kids, it can affect people of any age. Teens and adults experience ARFID, too, either as an eating disorder that begins later in life, or one that developed in childhood and was never treated. If you’re recognizing long-standing restrictive eating patterns in yourself, know that ARFID in adults is real, even if the diagnosis wasn’t widely discussed when you were younger.
ARFID vs. picky eating at a glance
On the surface, ARFID and picky eating can look similar: limited foods, strong preferences, pushback at meals. The key difference is how much that pickiness affects health and life, according to Jones.
“The primary distinguishers between ARFID and picky eating are the degree of selectivity and the impact of the selective eating. An individual who is a picky eater will often still eat at least a few foods in each of the basic food groups,” she says. “Someone who has selective eating due to ARFID often has few or no foods represented in at least one of the basic food groups.” And over time, their list of accepted foods generally shrinks, rather than expanding.
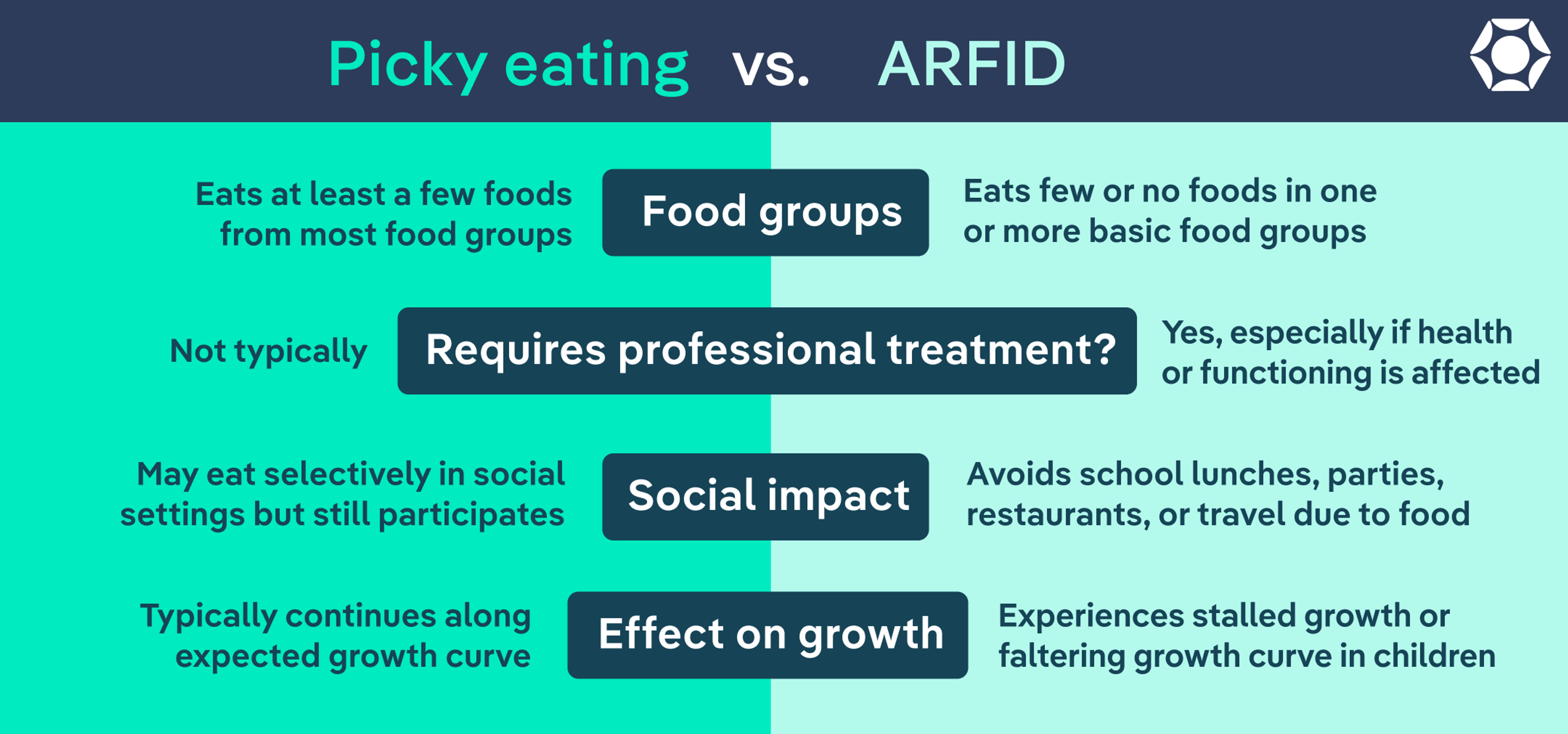
Here’s a side-by-side comparison to help you tell the difference between ARFID and picky eating, in yourself or a loved one:
Feature | ARFID | Picky Eating |
Age of onset | Can begin in childhood (sometimes as early as age 4) and persist into adolescence or adulthood | Most common in toddlers and preschoolers; often improves with age |
Variety of foods | Very limited list of safe foods, often shrinking over time | Limited preferences, but usually stable or gradually expanding |
Food groups | Few or no foods in one or more basic food groups | At least a few foods from most food groups |
Response to new foods | Intense distress, panic, gagging, or refusal | Reluctant but may try with low-pressure exposure |
Effect on growth | Weight loss, stalled growth, or faltering growth curve in children | Typically continues along expected growth curve |
Nutritional impact | Nutritional deficiencies or reliance on supplements | Usually nutritionally adequate overall |
Anxiety around eating | High anxiety, fear of choking/vomiting, strong sensory aversions | Mild frustration or dislike, but not overwhelming fear |
Social impact | Avoids school lunches, parties, restaurants, and travel due to food | May eat selectively in social settings but still participates |
Improves with time? | Often becomes more restrictive without intervention | Often improves gradually with development |
Requires professional treatment? | Yes, especially if health or functioning is affected | Not typically |
Warning signs that suggest ARFID (not picky eating)
It’s normal to second-guess yourself. Many parents wonder if they’re overreacting—or, on the flip side, if they’ve missed something important. The clearest signal for when to worry about picky eating is impact: is your child’s eating affecting their health, growth, or ability to participate in everyday life?
According to Jones and Ruberti-Bruning, here are some red flags that may suggest ARFID rather than typical picky eating:
- Significant weight loss or stalled growth: When someone isn’t gaining weight as expected, is losing weight, or has dropped off their growth curve.
- Nutritional deficiencies: Bloodwork shows low levels of key nutrients, or there are physical signs of malnutrition.
- Reliance on supplements: When someone depends on nutritional drinks or supplements to meet basic calorie or nutrient needs.
- A very limited (and shrinking) list of safe foods: Only a handful of foods feel acceptable, and that list gets smaller over time.
- Extreme distress around meals: Intense anxiety, tantrums, or panic when presented with certain foods.
- Gagging when exposed to certain foods: Strong food texture sensitivity or food aversion that triggers a physical reaction.
- Fear of choking or vomiting: Avoidance driven by worry that something bad will happen if they eat.
- Avoidance of social eating: Skipping parties, school lunches, sleepovers, or travel because of food.
- Little to no interest in food: Eating feels like a chore; hunger cues are low or absent.
- Sleep issues: Difficulty falling or staying asleep, poor sleep, or fatigue may be linked to inadequate nutrition.
If you’re noticing several of these signs in yourself or your child, it doesn’t mean you’ve done something wrong. It doesn’t mean you should have “fixed it sooner.” It simply means it may be time for more support than home strategies alone can provide.
Types of ARFID
Not everyone with ARFID struggles with food in the same way. In fact, there are three primary types of ARFID, and many people experience a mix of more than one. Here’s the breakdown.
Sensory-based avoidance
This type of ARFID is often what people picture when they think of extreme picky eating.
Here, eating is limited because of heightened sensitivity to the sensory properties of food: taste, texture, smell, temperature, or even color, says Jones. Certain textures may trigger gagging. Mixed foods may feel unbearable. A slight change in preparation can make a once-safe food suddenly feel impossible.
It’s also important to say this clearly: Sensory sensitivity on its own does not equal an eating disorder. Many neurodivergent individuals, such as those with autism or ADHD, experience sensory processing challenges. ARFID only becomes a concern when that sensitivity leads to nutritional gaps, weight changes, or major disruptions to daily life.
Fear-based (aversive) avoidance
In this type of ARFID, restriction is driven by fear rather than food preference.
“[Someone] limits the volume and/or variety of food out of fear that something negative will occur as the result of eating, such as vomiting, choking, allergic reaction, or pain,” explains Jones. “This response often begins following a food-related traumatic experience, such as an illness or choking incident.”
In these cases, anxiety is in the driver’s seat—and simply telling someone to “just try it” doesn’t address the fear underneath.
Lack of interest or low appetite
This type of ARFID can be harder to recognize because it doesn’t always involve strong dislikes or panic.
Instead, “there is little interest in food and a lack of appetite,” explains Ruberti-Bruning. “A person can go a long time without eating and experiences little to no joy in eating.”
Lack-of-interest ARFID can also include low hunger cues and early fullness, so the body doesn’t send strong signals to eat and feels full sooner than it should, adds Jones.
Even without dramatic food refusal, this pattern can still lead to weight loss, stalled growth, or nutritional deficiencies over time.
Mixed presentation
Many people don’t fit neatly into one category, says Jones. Someone might have sensory sensitivities and fear of choking, or low appetite combined with intense texture aversion.
The important takeaway is this: ARFID isn’t one-size-fits-all. The common thread is the impact on health and daily functioning.
When should you seek professional support?
One of the biggest differences between picky eating and ARFID shows up over time:
With typical picky eating, you generally see gradual improvement. A child might go through a phase of refusing certain foods, but their overall growth stays on track. The list of accepted foods may be limited, but it usually stays stable or slowly expands with low-pressure exposure and maturity. Social eating can be selective, but it doesn’t consistently prevent participation.
With ARFID, the pattern tends to intensify instead of soften. According to Jones and Ruberti-Bruning, here are some signs it may be time to seek professional support:
- Ongoing weight loss or slowed growth: Your child isn’t gaining weight as expected or has fallen off their growth curve.
- Nutritional deficiencies: Bloodwork or physical symptoms suggest gaps in essential nutrients.
- Heavy reliance on supplements: Nutritional drinks or supplements are needed to maintain weight or meet daily needs.
- Escalating anxiety around meals: Panic, meltdowns, or intense fear show up consistently at mealtimes.
- A shrinking list of safe foods: Variety decreases over time instead of expanding.
- Avoidance of social eating: School lunches, parties, restaurants, or travel are skipped because of food.
- Low appetite with medical impact: Persistent lack of hunger or early fullness is affecting weight, growth, or energy.
You don’t have to wait until things feel extreme to get support. Seeking an evaluation isn’t overreacting; it’s gathering information. And getting support early can protect you or your child’s health, ease family stress, and create a clearer path forward.
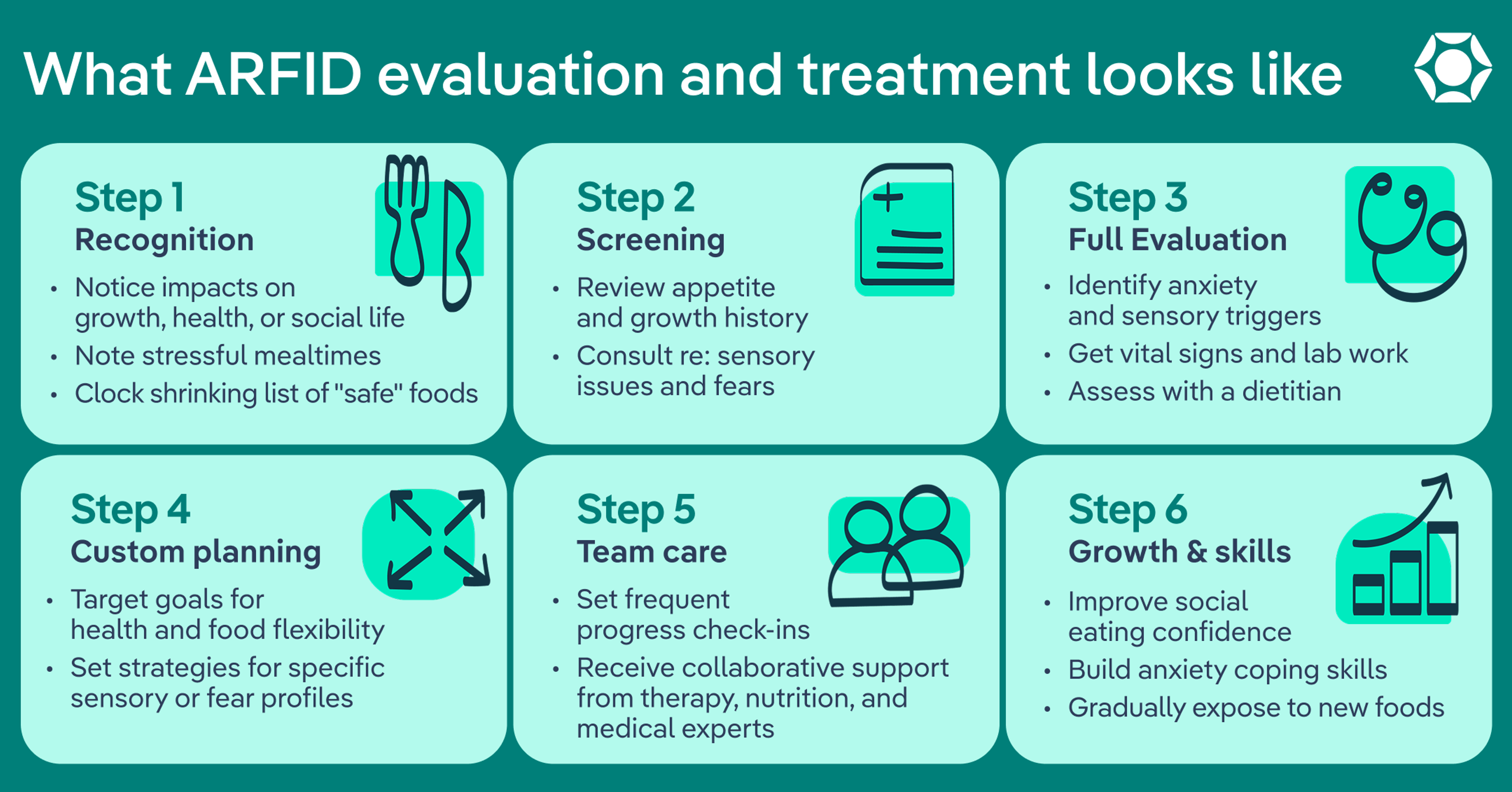
How is ARFID evaluated?
A thoughtful ARFID evaluation should feel thorough, collaborative, and specific, not dismissive. Here’s what to expect:
- Talking through eating history: A provider will ask about current safe foods, how the list has changed over time, portion sizes, appetite patterns, mealtime behavior, sensory sensitivities, and any fears related to eating.
- Reviewing growth and medical history: For kids and teens, providers will look at the bigger picture: how height and weight have changed over time. They may also order lab work to check for nutritional deficiencies or other health concerns, just to make sure the body is getting what it needs.
- Assessing psychosocial impact: Food doesn’t exist in a vacuum. A good evaluation will explore how eating is affecting everyday life. Is your child avoiding school lunch? Skipping birthday parties? For adults, is work travel stressful because of food? If eating is shrinking someone’s world, that matters.
- Screening for co-occurring conditions: ARFID can overlap with conditions like anxiety, ADHD, autism, or gastrointestinal conditions. Your provider will consider the full picture in order to guide the right kind of support.
- Determining what kind of support is needed: If someone’s health is at risk—like significant weight loss or dehydration—your doctor may recommend inpatient treatment at first to address any acute medical issues. For many people, though, treatment can happen through regular outpatient appointments. Either way, a thoughtful provider will make sure the level of support matches what the body and brain need right now.
Because ARFID is a relatively newer diagnosis, not all providers are trained to recognize it. That’s why it’s important to work with an ARFID-informed clinician or team who understands the nuances of restrictive eating that isn’t driven by body image. If you’re unsure where to start, this ARFID self-assessment can help clarify next steps.
ARFID treatment also requires collaboration, says Ruberti-Bruning. A registered dietitian who specializes in ARFID, a therapist, and a doctor or pediatrician are all key members of the team.
What does treatment for ARFID look like?
The good news is that ARFID is treatable. Equip is the largest ARFID treatment provider in the U.S., and has a wide variety of ARFID-specific support. And rest assured, treatment doesn’t require forcing foods, issuing ultimatums, or turning meals into battles. Instead, it’s structured, gradual, and tailored to the specific reasons behind the restriction.
According to Jones and Ruberti-Bruning, here’s what that support usually involves:
- A team approach: Most people work with a multidisciplinary team that includes a therapist, a dietitian, and a medical provider. The therapist helps address anxiety, fear, or rigidity around food. The dietitian helps make sure nutritional needs are met and guides the process of expanding foods. A medical provider keeps an eye on growth, labs, and overall health. Everyone works together.
- Gradual exposure to new foods: One of the core parts of treatment is slowly, carefully expanding the range of foods someone can eat. That might mean trying a new version of a familiar food. Or taking one small bite of something new. The pace is slow and steady to help someone build confidence around new foods.
- Support for anxiety or fear: If eating feels scary, therapy focuses on helping the brain feel safer around food. Over time, that fear response can soften. Cognitive-behavioral therapy for ARFID (CBT-AR) is one evidence-based approach specifically designed for this. It helps identify the patterns keeping avoidance in place and gently challenges them through small, supported steps. Over time, that fear response can soften, and eating can start to feel more manageable.
- Caregiver involvement: For children and teens with ARFID, parents or caregivers play a central role in treatment. In family-based therapy (FBT), caregivers are supported and coached to take an active role in helping their child eat more consistently and gradually expand their range of foods at home. Rather than placing the responsibility on the child alone, FBT empowers families with tools, structure, and guidance—making them a key part of the recovery process.
- Building structure around meals: Sometimes eating has become so unpredictable that the body’s hunger cues are out of sync. That’s why treatment may include setting regular meals and snacks to help the body relearn when to expect food.
- Addressing the whole picture: If anxiety, ADHD, autism, or medical issues are also part of the story, those are addressed too.
Progress is usually gradual. Expanding food variety takes time. But many families begin to notice something shifts before the food list dramatically grows: The stress decreases. Meals feel less explosive. Fear loosens its grip.
ARFID isn’t a character flaw. It’s a real eating disorder with real physical and emotional impacts. Treatment centers on helping someone feel safe around food again, supported through the process, and adequately nourished so their body and brain can grow and thrive.
The bottom line
Picky eating is common, especially in young kids. ARFID, on the other hand, is restrictive eating that affects health, growth, nutrition, or daily life—and it often becomes more restrictive over time.
If you’re worried, trust that instinct. ARFID is treatable, and early, informed support can reduce stress and protect both physical and emotional health. You don’t have to wait until things feel extreme to reach out for clarity and next steps.
Frequently asked questions (FAQs)
What is the difference between being picky and having ARFID?
Picky eating usually involves strong preferences but doesn’t significantly affect growth, nutrition, or daily life. Many picky eaters still eat from most food groups and gradually expand their foods over time.
ARFID is an eating disorder involving restrictive eating that leads to meaningful consequences. That includes weight loss or stalled growth, nutritional deficiencies, reliance on supplements, or avoidance of social situations because of food. Put simply, the biggest difference between ARFID and picky eating is impact.
What are the three types of ARFID?
There are three main types of ARFID, though many people experience a mix of more than one type:
- Sensory-based avoidance: Restriction driven by heightened sensitivity to taste, texture, smell, or other sensory qualities.
- Fear-based (aversive) avoidance: Restriction driven by fear of choking, vomiting, allergic reactions, or other negative outcomes.
- Lack of interest or low appetite: Limited intake due to low hunger cues or minimal interest in food.
Do kids grow out of ARFID?
ARFID usually doesn’t fade on its own the way typical picky eating often does as a child matures. Without support, eating patterns can become more rigid over time, not less. The earlier someone gets help, the easier it is to expand foods, lower anxiety around meals, and prevent bigger health concerns in the future.
What do people with ARFID usually eat?
People with ARFID often rely on a limited number of foods. ARFID safe foods may be very specific in brand, texture, or preparation. For example, someone might only eat a certain type of pasta prepared in a particular way, or avoid entire food groups because of sensory discomfort or fear. Over time, the list of safe foods may shrink without treatment.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders : DSM-IV-TR. 4th ed., Washington, DC, American Psychiatric Association, 2000.
Menzel, Jessie E, and Taylor R Perry. “Avoidant/Restrictive Food Intake Disorder: Review and Recent Advances.” Focus (American Psychiatric Publishing) vol. 22,3 (2024): 288-300. doi:10.1176/appi.focus.20240008
Passarello N, Tarantino V, Chirico A, et al. Sensory Processing Disorders in Children and Adolescents: Taking Stock of Assessment and Novel Therapeutic Tools. Brain Sci. 2022;12(11):1478. Published 2022 Oct 31. doi:10.3390/brainsci12111478
Pjetraj, Dorina et al. “Decoding Picky Eating in Children: A Temporary Phase or a Hidden Health Concern?.” Nutrients vol. 17,24 3884. 12 Dec. 2025, doi:10.3390/nu17243884
Ramirez, Zerimar, and Sasidhar Gunturu. “Avoidant Restrictive Food Intake Disorder.” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK603710/.
Seetharaman, Sujatha, and Errol L Fields. “Avoidant/Restrictive Food Intake Disorder.” Pediatrics in review vol. 41,12 (2020): 613-622. doi:10.1542/pir.2019-0133
Thomas, Jennifer J et al. “Cognitive-behavioral therapy for avoidant/restrictive food intake disorder: Feasibility, acceptability, and proof-of-concept for children and adolescents.” The International journal of eating disorders vol. 53,10 (2020): 1636-1646. doi:10.1002/eat.23355
Van Wye, Eliza et al. “Protocol for a randomized clinical trial for Avoidant Restrictive Food Intake Disorder (ARFID) in low-weight youth.” Contemporary clinical trials vol. 124 (2023): 107036. doi:10.1016/j.cct.2022.107036









