What Causes ARFID? Understanding the “Why” Behind Avoidant Eating


- ARFID doesn’t have a single cause. It usually develops from a mix of biological, environmental, and psychological factors that build on each other.
- ARFID is not driven by body image concerns or a desire to lose weight, which is what separates it from many other eating disorders.
- Common underlying drivers include sensory sensitivities, how your body signals hunger, and how your brain responds to fear or anxiety around eating.
- ARFID is not a choice or a phase. Understanding the “why” behind the condition can help you take the next step towards support.

Maybe your child only eats a small number of foods or reacts strongly to certain textures. Perhaps your meals feel stressful, or eating just doesn’t come easily. If that sounds familiar, you’re not imagining it, and you’re not alone. For some people, these patterns are part of an eating disorder called avoidant/restrictive food intake disorder (ARFID). But what causes ARFID?
Like all eating disorders, ARFID doesn’t have a single cause—it typically develops from a mix of biological, environmental, and psychological factors. One thing that makes ARFID different, though, is that it isn’t driven by body image or a desire to lose weight. It’s often shaped by things like sensory sensitivities, differences in appetite, and fear or anxiety around eating.
Below, we’ll break it all down so you can better understand what might be driving these eating patterns—and that recovery is possible.
What causes ARFID?
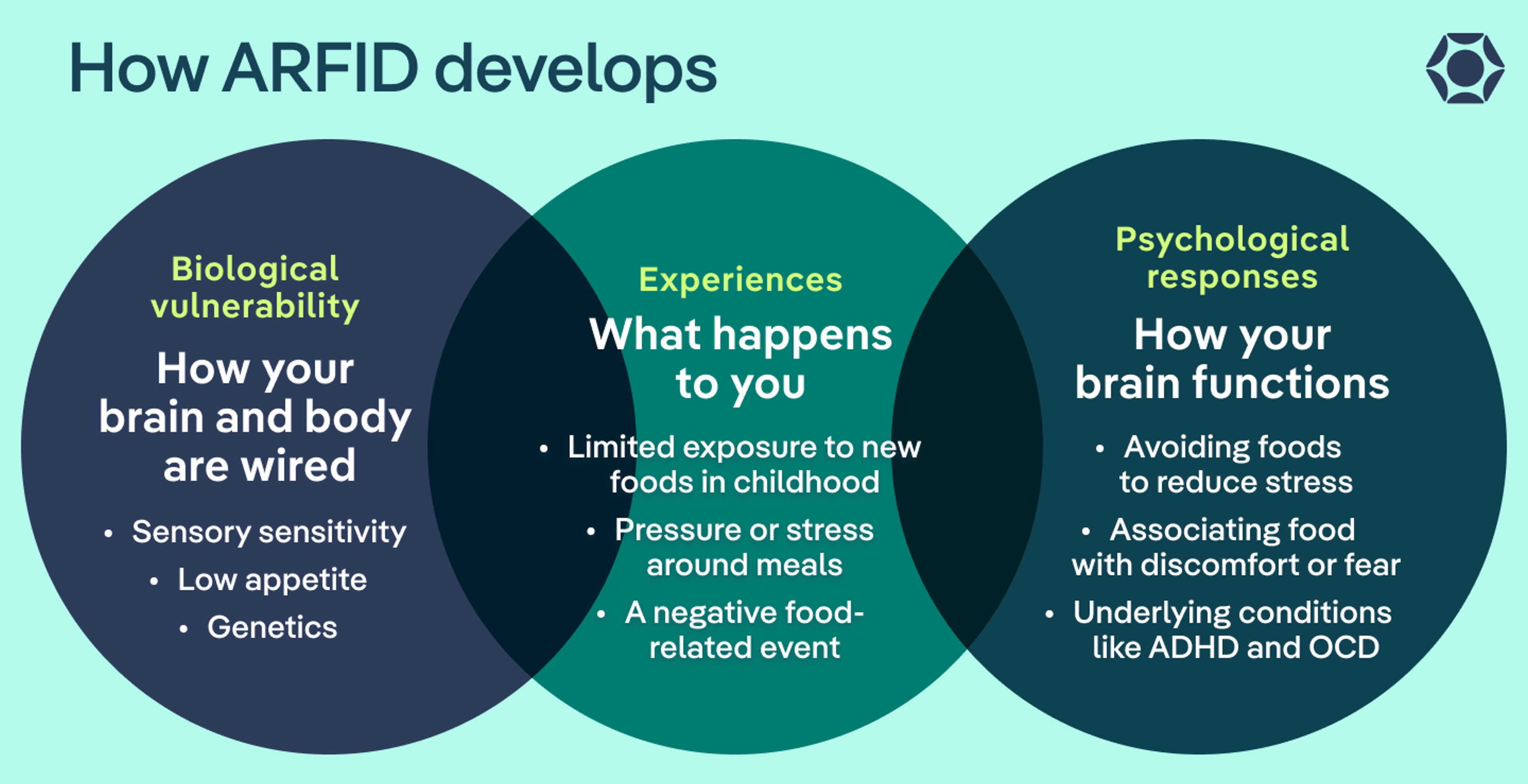
ARFID isn’t caused by one single thing. Most of the time, it stems from a combination of factors, according to Michelle Jones, PhD, a clinical instructor at Equip. While the research is still evolving, Jones says these can include:
- Biological vulnerability: Research suggests there may be an inherited component to ARFID, meaning some people are more likely to have traits like heightened sensory sensitivity or a low appetite. For them, eating can feel overwhelming, unappealing, or harder to tune into from the start.
- Experiences: Experiences like limited exposure to new foods, pressure at mealtimes, or a specific event that made eating feel unsafe can contribute to ARFID.
- Psychological responses: If eating has felt uncomfortable or scary, the brain can start to interpret food as something to avoid, reinforcing patterns of anxiety and restriction. How your brain functions at baseline can play a role, too. For instance, conditions like autism, ADHD, anxiety, and OCD can make someone more sensitive to food, more rigid in their thinking, or less in tune with hunger and fullness cues.
Biological contributors to ARFID
“While there are certainly environmental and experiential contributors to the development of ARFID … current research suggests that biological and genetic factors play a significant role,” says Jones.
In other words, ARFID isn’t a choice. So if you notice these patterns in yourself or someone you care about, there’s a reason behind them—they’re often rooted in real differences in how the body and brain respond to food. Here’s how that can show up.
Genetics
Researchers are still learning about the role genetics play in ARFID. What we do know so far is that some people may be more biologically predisposed to developing eating disorders, including ARFID.
That’s not to say someone is born with ARFID itself. But it can mean they’re wired in a way that makes them more vulnerable to the condition. From there, other factors can build on that foundation and shape how ARFID develops over time.
Sensory sensitivities to food
“ARFID is often misunderstood as ‘picky eating,’ but it is much more complex,” says Lily Thrope, LCSW, founder of Thrope Therapy.
For some people, that complexity starts with how their body processes sensory input. They may be “biologically predisposed to detect more minute changes in taste, texture, and other sensory properties of foods,” explains Jones. This is especially true with food aversions for people on the autism spectrum, she adds.
In practice, sensory sensitivity ARFID means that foods that might seem neutral to someone else can feel intensely unpleasant or even intolerable. For example, a mushy texture, mixed foods, or strong smells might trigger a physical reaction like gagging or a strong feeling of disgust.
Differences in appetite and hunger cues
Not everyone experiences hunger the same way. For some people, the part of the brain that regulates appetite works differently, which can cause low appetite. These patterns can show up as early as infancy, says Jones. This might look like:
- Lack of interest in food
- Forgetting to eat
- Feeling full quickly
- Not thinking about food very often
These differences can contribute to lack of interest ARFID, the type of ARFID in whichsomeone is not eating enough because the body doesn’t send clear, consistent hunger signals.
Gastrointestinal discomfort and physical symptoms
Physical discomfort can also play a role. After all, if eating regularly leads to stomach pain, nausea, reflux, or other unpleasant symptoms, it makes sense that food can start to feel stressful or scary.
And even if the discomfort isn’t severe, those repeated experiences can add up. Over time, the brain and body start to associate eating with feeling unwell. From there, it’s natural to pull back (whether that means avoiding certain foods or eating less overall).
Environmental and experiential contributors to ARFID
Another important piece of the puzzle is someone’s experience with food.
In some cases, a single distressing event with eating can play a major role in the onset of ARFID. In others, it’s a combination of repetitive experiences and environmental factors.
Regardless, these moments tend to interact with patterns that are already there (like a naturally low appetite or eating habits adopted due to underlying gastrointestinal disease), shaping how someone relates to food over time, says Jones.
In other words, certain experiences can either reinforce a sense of safety around food, or the opposite. Here are some common examples.
Early feeding experiences
Early experiences with food can leave a lasting imprint, even if they seem small at the moment.
For example, if a child doesn’t have many chances to explore new foods, they may not build the familiarity that helps those foods feel safe. Over time, new foods can start to feel unpredictable or overwhelming.
At the same time, pressure to eat can backfire, says Jones. Being pushed or forced to eat foods that feel uncomfortable can turn meals into a stressful experience.
Negative food-related events
For some people, ARFID begins after a specific experience that made eating feel unsafe, like:
- Choking
- Food poisoning
- Gastrointestinal illness
- Allergic reaction
After something like that, it’s completely understandable for the brain to go into “better-safe-than-sorry” mode.
As a result, foods that once felt fine can start to feel risky. And for some people, that sense of caution can stick—and grow—over time, changing how safe or manageable eating feels moving forward.
Family and environmental influences
The environment around food matters more than people often realize. According to Thrope, everyday moments can shape someone’s experience of eating well into the future, including:
- How your family or community talks about food
- Whether meals feel calm or tense
- The effects of food insecurity, like unpredictable or limited access to food
Psychological contributors to ARFID
The final piece of the puzzle is how the brain responds to all of these factors.
Over time, the brain starts to connect the dots. If eating feels unsafe, it begins to treat food as something to be cautious about (or avoid altogether). And even when the original trigger is gone, that reaction can stick. Here’s how that can play out.
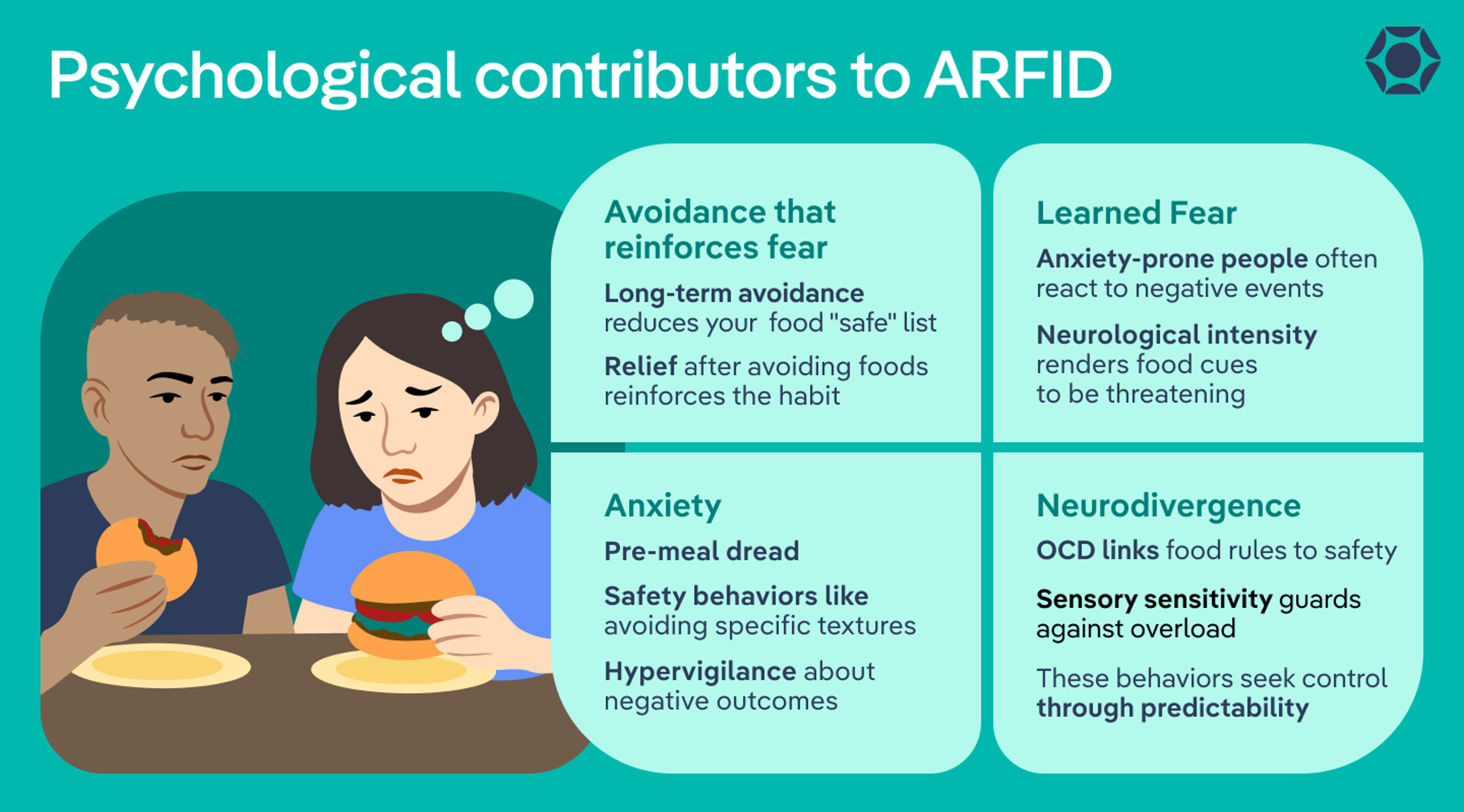
Anxiety
Anxiety plays a big role for many people with ARFID—in fact, research has found links between ARFID and anxiety disorders.
Here’s why: If eating has felt uncomfortable, unpredictable, or scary, the brain can start to stay on high alert around food. It’s trying to do its job: Keep you safe. But sometimes it gets a little overprotective.
That can show up as:
- Feeling anxious before or during meals
- Avoiding certain foods or situations where eating feels uncertain
- Overthinking bad things that could happen
Learned fear
The brain is really good at learning from experience … especially negative ones.
If something distressing happens around food, the brain takes note as a way to protect you from it happening again. Over time, it can start to associate that food with danger.
Research also suggests this fear can show up in the brain itself. Studies have found that the brain regions involved in emotion, attention, and sensory processing respond more strongly to food cues in people with ARFID. Put simply, that means food can feel more intense, overwhelming, or even threatening on a neurological level.
And for some people, that response is stronger than others. “Individuals predisposed to anxiety may be more likely to experience ARFID symptoms following [negative] events compared to those who are not predisposed to anxiety,” says Jones.
Avoidance that reinforces fear
Here’s where things can start to snowball. If a food feels scary or uncomfortable, avoiding it brings immediate relief, says Thrope. And that relief sends a clear message to the brain: Good call, let’s keep doing that.
In the short term, it helps ease discomfort. In the long term, it can make things harder. The more a food is avoided, the more unfamiliar it becomes—and the more intense the reaction can feel the next time it comes up. This is how the list of “safe” foods can slowly get smaller over time.
Neurodivergence
How someone’s brain is wired can also shape how all of this plays out.
“People with ADHD, autism and other neurodivergence often struggle with sensory sensitivity, which can relate to fear around certain sensory experiences of food,” explains Thrope. “[This] can often look like rigidity or control, but is often related to something deeper like a fear or sensory avoidance.”
ARFID and OCD are also linked. Some people develop very strong fears or specific rules around food that feel important to follow. These patterns are the brain’s way of trying to create a sense of safety and control.
If this sounds familiar, you’re not broken. These responses are rooted in how the brain processes information and tries to keep things predictable and safe.
What ARFID is not caused by
When you’re trying to make sense of the symptoms of ARFID, it’s easy to look for something—or someone—to blame. But ARFID isn’t caused by a single mistake or shortcoming. It’s also not driven by many of the things people often assume, like:
- Bad parenting: While early experiences with food can shape eating patterns, they don’t cause ARFID on their own. Many caregivers are simply responding to a child who is already struggling by doing what feels most helpful in the moment.
- Picky eating: While it can be hard to distinguish ARFID versus picky eating on the surface, they’re not the same thing, says Thrope. Picky eating is common in childhood and often temporary. ARFID tends to be more severe, longer-lasting, and tied to deeper underlying factors.
- Body image: Unlike many other eating disorders, ARFID isn’t driven by a desire to lose weight or change appearance, says Jones. Instead, the restriction comes from how eating makes someone feel.

How ARFID develops over time
Remember, ARFID typically develops when multiple factors collide. Because of that, ARFID in children builds gradually—sometimes starting as early as infancy or toddlerhood and becoming more noticeable as eating patterns take shape, according to Jones.
For example, she says a child might be sensitive to food textures and have strong reactions to certain foods. To keep meals manageable, caregivers may stick to a small set of ARFID “safe” foods. Over time, that can mean fewer chances to try new foods, and unfamiliar foods can start to feel more overwhelming.
In adults, ARFID can look a little different. It may show up after a specific event, like GI surgery or an allergic reaction. After something like that, it’s completely understandable for the brain to shift into protection mode and start linking food with danger.
Even then, it’s usually not just the event itself. Underlying factors—like anxiety, sensory sensitivity, or appetite differences—can make that response stronger and more likely to stick.
For example, someone might get food poisoning and start to feel anxious about eating. Even after they recover, that association can linger. They may begin avoiding certain foods, then more foods, and eventually rely on a narrow set of options.
The bottom line
ARFID doesn’t come from a single cause. It develops from a mix of factors, including how someone is wired, what they’ve experienced, and how their brain responds to it all
That’s why it can look so different from person to person. It’s also why it’s not something someone can just “push through”—ARFID is rooted in real biological and psychological differences, not a lack of effort or willpower.
Put simply, there’s a reason eating feels this way, and you’re not alone in it. These patterns make sense when you understand what’s driving them, and with the right kind of support, recovery is absolutely possible. If you’re wondering whether ARFID might be part of you or your child’s experience, taking a quick screener can be a low-pressure first step toward getting clarity and support.
Frequently asked questions (FAQs)
Are you born with ARFID or can you develop it?
You’re not born with ARFID itself, but you can be born with traits that make it more likely to develop (like sensory sensitivity or low appetite). From there, experiences and learned responses can shape how eating patterns develop over time.
How does ARFID develop?
There are a number of causes of ARFID. It often develops as the result of a combination of biological traits (like difficulty reading hunger cues), experiences with food (like pressure at meals or a negative event), and how the brain responds over time (like anxiety or avoidance). In children, this tends to build gradually. In adults, it can sometimes start after a specific trigger.
What causes ARFID in adults?
ARFID in adults often develops after a specific trigger, like choking, food poisoning, or a gastrointestinal illness. But underlying factors—like anxiety, sensory sensitivity, or appetite differences—usually play a role in how those patterns take hold and persist.
Deep dive recommendations
If you want to learn more or find additional support, these trusted resources can help:
- Equip: In-depth articles, treatment information, and support options
- Feeding Matters: Resources on feeding challenges, including ARFID
- F.E.A.S.T. (Families Empowered and Supporting Treatment of Eating Disorders): Guidance and support for families
- National Eating Disorders Association (NEDA): Education, screening tools, and support resources
Białek-Dratwa, Agnieszka et al. “Food Neophobia and Avoidant/Restrictive Food Intake among Adults and Related Factors.” Nutrients vol. 16,17 2952. 2 Sep. 2024, doi:10.3390/nu16172952
Bjørndal, Ludvig Daae et al. “Prevalence, Characteristics, and Genetic Architecture of Avoidant/Restrictive Food Intake Phenotypes.” JAMA pediatrics vol. 180,1 (2026): 45-55. doi:10.1001/jamapediatrics.2025.4786
Bulik, Cynthia M et al. “Arfid Genes and Environment (ARFID-GEN): Study Protocol.” Research square rs.3.rs-3186174. 31 Aug. 2023, doi:10.21203/rs.3.rs-3186174/v1. Preprint.
Che, Yunqiu et al. “Avoidant/Restrictive Food Intake Disorder in Adult Patients with Gastrointestinal Diseases: A Concept Analysis Using Evolutionary Approach.” Risk management and healthcare policy vol. 18 2063-2080. 21 Jun. 2025, doi:10.2147/RMHP.S520802
Di Cara, Marcella et al. “Avoidant Restrictive Food Intake Disorder: A Narrative Review of Types and Characteristics of Therapeutic Interventions.” Children (Basel, Switzerland) vol. 10,8 1297. 28 Jul. 2023, doi:10.3390/children10081297
Di Luzio, Michelangelo et al. “Understanding the Relationship Between Avoidant/Restrictive Food Intake Disorder and Obsessive-Compulsive Symptoms: A Systematic Review.” Nutrients vol. 18,5 874. 9 Mar. 2026, doi:10.3390/nu18050874
Henriksen, Sissel Bekker et al. “Avoidant-Restrictive Food Intake Disorder in Patients With Gastrointestinal Disorders: A Systematic Review.” Journal of human nutrition and dietetics : the official journal of the British Dietetic Association vol. 39,2 (2026): e70226. doi:10.1111/jhn.70226
Laboe, Agatha A et al. “The relation of food insecurity to eating disorder characteristics and treatment-seeking among adult respondents to the National Eating Disorders Association online screen.” Eating behaviors vol. 50 (2023): 101776. doi:10.1016/j.eatbeh.2023.101776
Menzel, Jessie E, and Taylor R Perry. “Avoidant/Restrictive Food Intake Disorder: Review and Recent Advances.” Focus (American Psychiatric Publishing) vol. 22,3 (2024): 288-300. doi:10.1176/appi.focus.20240008
Ramirez, Zerimar, and Sasidhar Gunturu. “Avoidant Restrictive Food Intake Disorder.” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK603710/.
Richson, Brianne N, and Hana F Zickgraf. “Lifetime and current mental health based on avoidant/restrictive food intake disorder history versus other eating disorder history in the Healthy Minds Study.” The International journal of eating disorders vol. 57,10 (2024): 1999-2005. doi:10.1002/eat.24218
Thomas, Jennifer J et al. “Avoidant/Restrictive Food Intake Disorder: a Three-Dimensional Model of Neurobiology with Implications for Etiology and Treatment.” Current psychiatry reports vol. 19,8 (2017): 54. doi:10.1007/s11920-017-0795-5
Thomas, Jennifer J et al. “Neural Response to Food Cues in Avoidant/Restrictive Food Intake Disorder.” JAMA network open vol. 8,2 e2460101. 3 Feb. 2025, doi:10.1001/jamanetworkopen.2024.60101
Watts, Rosie et al. “The clinical presentation of avoidant restrictive food intake disorder in children and adolescents is largely independent of sex, autism spectrum disorder and anxiety traits.” EClinicalMedicine vol. 63 102190. 30 Aug. 2023, doi:10.1016/j.eclinm.2023.102190









