What Causes Eating Disorders?


- The causes of eating disorders are complex and include an interplay of biological, psychological, and social factors.
- Recovery is possible even if you don’t know the exact cause of someone’s eating disorder.
- Treatment is available and recovery is possible with the help of a knowledgeable care team.

In my 20s, a therapist diagnosed me with “eating disorder not otherwise specified (EDNOS),” now called otherwise specified feeding or eating disorder (OSFED). On the outside, I looked healthy and fit. But a closer look would have revealed a person restricting her food while also engaging in extreme endurance exercise. To anyone unfamiliar with eating disorder causes, my behavior probably suggested I wanted to lose weight, even though I was already thin.
But that was not the driver of my disordered behavior. I had been diagnosed with several chronic illnesses at a young age and was in and out of the hospital, including the intensive care unit. Then in early adulthood, I received another diagnosis: endometriosis, a condition that’s associated with an increased risk of developing an eating disorder.
Chronic pain and a host of other unpredictable symptoms disrupted my life to the point where I felt I had no control. So I attempted to exert control by restricting food well below what I needed to support my physical activity level.
This is just my experience, but my situation illustrates how complex eating disorders can be. Although body image can play a role, it doesn’t always, and many different factors are usually at play. In this article, we explore causes of eating disorders, eating disorder triggers, and more.
The biopsychosocial model of eating disorders
Each of us has a unique set of life experiences, personality traits, and genetics. And all these factors (and more) can contribute to developing an eating disorder.
Researchers have come up with a basic model for explaining what causes eating disorders, called the biopsychosocial model. It illustrates that eating disorder causes are not one-size-fits-all and that multiple factors overlap, creating a perfect storm that leads to the illness developing.
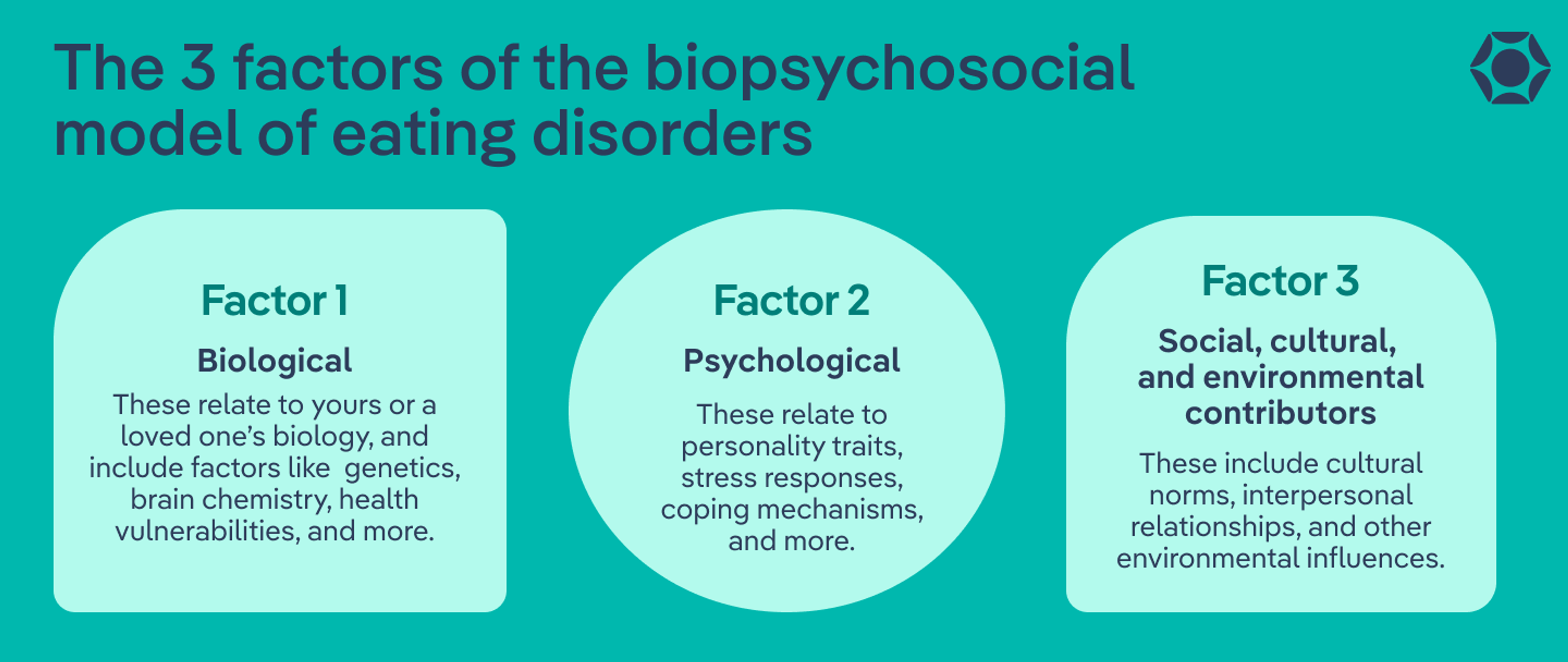
This model suggests that eating disorders are caused by an interplay of three categories of factors:
- Biological contributors: These relate to yours or a loved one’s biology, and include factors like genetics, brain chemistry, health vulnerabilities, and more.
- Psychological contributors: These relate to personality traits, stress responses, coping mechanisms, and more.
- Social, cultural, and environmental contributors: These include cultural norms, interpersonal relationships, and other environmental influences.
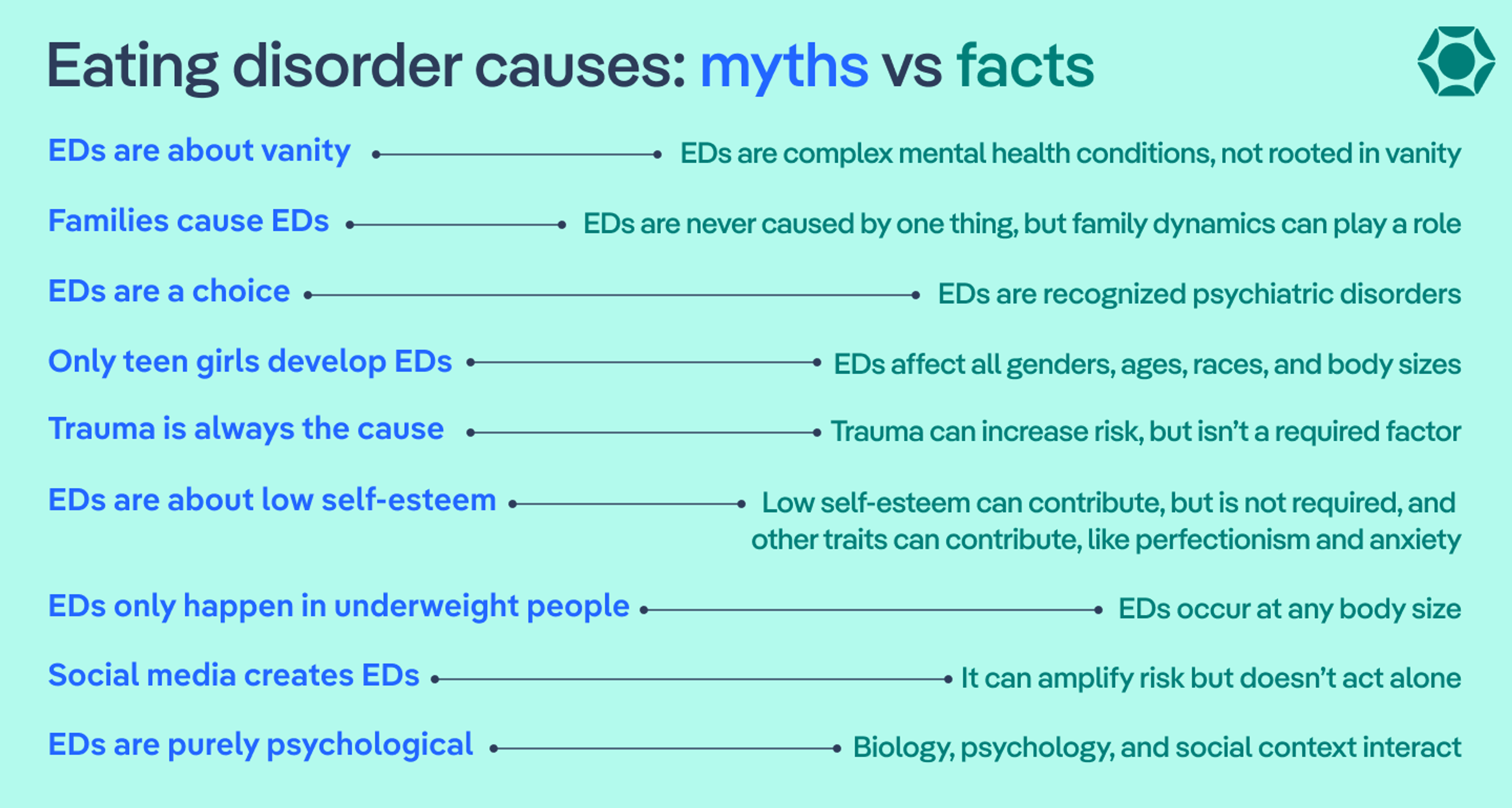
We explore each of these categories in depth below. But first, let’s bust through a few myths about eating disorder causes.
Eating disorder causes vs triggers
Before we explore the causes of eating disorders, it’s important to differentiate between causes and triggers. “Causes are the deeper vulnerabilities someone may carry, while triggers are the moments that turn up the volume,” says Dr. Melodie Simmons, a licensed professional counselor and certified eating disorder specialist-consultant at Equip.
For example, you might have certain personality traits that increase your vulnerability to developing an eating disorder—but just because you’re more likely to develop one doesn’t mean you will. The eating disorder only “switches on” when there is a trigger, such as trying an overly restrictive diet. And if you or a loved one already has an eating disorder, then triggers may exacerbate it.
Although I’m recovered, I still consider myself to have OSFED. I used to try to control the number on the scale, so I know that weighing myself is triggering for me. For this reason, when I go to the doctor and the intake nurse asks me to step on the scale, I decline unless my current weight is necessary to determine a medication dosage. Even then, I ask for the nurse not to tell me my weight.
Biological and genetic contributors
Now let’s explore the three elements of the biopsychosocial model, starting with biological causes of eating disorders. Based on genetics and other biological factors, you or a loved one may have inherited a vulnerability to developing an eating disorder. Additionally, chemical messengers in the body, such as neurotransmitters and hormones, can play a role, as can structural differences in brain regions. Plus, how your body manages energy balance also factors in.
Remember, none of these factors make you or a loved one flawed, and they are out of your control.
Genetics and family history
Various studies have looked at twins and other family members and have explored whether certain gene variants contribute to eating disorder vulnerability. Through these studies, research shows that inherited factors account for 28% to 84% of eating disorder risk. Although more research is needed, some studies have found that variations in our family genes can make us more likely to develop an eating disorder.
Brain chemistry and hormones
Neurotransmitters and hormones act as chemical messengers in the body and brain. Differences in these chemical messengers can be inherited or may develop for other reasons, and they can play a role in eating disorders. Here are some examples.
- Serotonin: This hormone and neurotransmitter helps regulate mood, appetite, and cognitive flexibility, or the ability to adapt your behavior to changing needs. Research shows that serotonin dysregulation and gene variants that affect serotonin pathways are both associated with eating disorders. Additionally, malnutrition, which can be an outcome of some eating disorders, can cause serotonin dysregulation and reinforce food restriction, creating a vicious cycle.
- Dopamine: This hormone and neurotransmitter is involved in motivation, reward, and other processes. Gene variants in the dopaminergic system may reinforce binging and/or purging cycles that are common with some eating disorders.
Energy balance
Your hormones also impact appetite, including whether you feel hungry or satisfied. Dysregulation with these hormones, including leptin and ghrelin, may contribute to eating disorder development.
- Leptin is a hormone that is produced in fat cells. It sends signals to the brain that you are satisfied when full. But leptin resistance can occur with high leptin levels. Leptin resistance means your brain ignores leptin's signals. Higher leptin (and potentially leptin resistance) is linked to binge eating disorder, though this is just one example.
- Ghrelin is “the hunger hormone.” It’s produced in your gastrointestinal tract and signals to your brain that you are hungry. Higher ghrelin is potentially implicated in several eating disorders.
Structural differences in brain regions
Our brains are made up of different regions and networks that work together, or separately, in complex ways. Although, as humans, we all have similar brain structures, no two brains are the same. Genetics, our experiences, and our behavior patterns all influence our brain structure.
Some structural differences contribute to various eating disorders, and these may be genetic or develop over time. Examples include gray and white matter changes, cortical and subcortical thickness differences, and network connectivity changes.
Our brains are made up of various networks. These networks connect different parts of the brain and help them work together. This connectivity is ever changing depending on which networks you’re using in a given moment. And if you were to compare your brain with mine, our networks would look a bit different. I like to think of it as no two snowflakes are the same. If you have an eating disorder, you may have enhanced connectivity in some areas and reduced connectivity in others.
Psychological contributors
Some underlying mental health conditions, personality traits, and even differences in cognitive processes can make you or a loved one more vulnerable to developing an eating disorder. Again, none of these psychological causes of eating disorders make you or a loved one flawed. These are some of the very factors that make us all unique. In fact, some of the personality traits that lead to an ED can, when channeled into something more productive and healthy, lead people to be extremely successful and happy.
Co-occurring mental health conditions
Eating disorders are mental health conditions themselves. But having a mental health condition—such as anxiety, depression, obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), substance use disorders, and more—can increase risk for developing an eating disorder.
Personality traits
Certain personality traits, including impulsivity, perfectionism, novelty-seeking, obsessive-compulsiveness, neuroticism, and avoidance are associated with eating disorders.
Dr. Simmons says these traits come up often. “But I’m careful not to pathologize those qualities,” she adds. “I’ll tell patients that nothing is wrong with their personality. The eating disorder just learned how to use their strengths in a rigid way. That shift helps reduce shame and builds compassion.”
As an example, although I’ve never had a formal diagnosis of OCD, I do have the trait of obsessive-compulsiveness. Though I didn’t have a term for it at the time, I first noticed this trait when in the ICU as a child. I feared for my life and thought that if I prayed a lot and “the right way,” I’d survive. I would start my prayers over if I did not do the sign of the cross perfectly.
When I developed disordered eating behaviors, my obsessive-compulsiveness traits “helped” me lock in on my rigid behaviors of doing everything I could to control the number on the scale.
Neurocognitive processes
How we navigate life is rooted in our neurocognitive processes. Neurocognitive processes include how we intake new information, store it, and retrieve it, and how we use that information for our thoughts and behaviors. Our neurocognitive processes include our executive function. This is the way your brain handles tasks and regulates your behaviors.
Everyone has unique ways of navigating life’s challenges, and your methods are likely a bit different from your best friend’s. However, some people are neurodiverse, which means their brain functions differently than what’s considered “normal,” usually referred to as neurotypical.
The conditions of attention-deficit hyperactivity disorder (ADHD) and autism are examples of neurodivergence, which can make you or a loved one more vulnerable to developing an eating disorder.
“Texture sensitivities, strong need for predictability, or difficulty sensing hunger and fullness can make eating feel genuinely overwhelming,” Dr. Simmons explains. “I frame neurodiversity as a difference, not a deficit, and adjust treatment so it honors how that person’s brain and body naturally work.”
Social, cultural, and environmental contributors
Social, cultural, and environmental factors are all interconnected. Here are few to consider.
Trauma
Eating disorders are more prevalent in people who’ve experienced trauma. Trauma at any time, including and especially in childhood, alters your stress response. These alterations can affect your brain chemistry and neurocognitive processes.
Trauma includes many things, such as sexual assault, any form of abuse, military combat, harrowing experiences such as surviving a natural or manmade disaster or a severe car accident, facing food insecurity or poverty in general, experiencing systemic racism in your community, severe illness, and more.
“Trauma can shape how someone experiences safety and control in their body,” Dr. Simmons says, “and sometimes eating disorder behaviors become ways to cope with overwhelming feelings. Trauma isn’t always part of the picture. Eating disorders are complex, and effective treatment usually means addressing both the nervous system and the behavioral patterns that keep it going.”
Living environment and upbringing
Do families cause eating disorders? This is a common question. And the answer isn’t straightforward. The short answer is, no, families do not directly cause eating disorders. But parents and other caregivers can influence a child’s relationship with food, exercise, and more. Negative associations can increase a person’s vulnerability to developing an eating disorder. However, the blame game isn’t useful and can even impede recovery.
Culture
The cultures you’re exposed to can also increase susceptibility to developing an eating disorder. The influences are many.
- Sports: Engaging in sports or physical activity is generally a healthy thing. And sports don’t directly cause eating disorders—however, the culture at play in sports can. For example, wrestlers may be encouraged to reach or maintain a certain weight by any means necessary, and the same is true of ballerinas or other dancers. That said, athletes in non-weight-sensitive sports are also at increased risk for eating disorders.
- Media: Eating disorders have existed for thousands of years. So media, including social media, isn’t a direct cause. However, media can certainly influence eating disorder development. Media often portrays whatever society considers the “ideal body” of the moment, and these portrayals can be an eating disorder catalyst.
- Diet culture: Related to media is the general concept of diet culture, in which society tends to champion thin bodies and assign morality to food, with certain foods being “good” and others “bad.” This culture sometimes links self-worth to body size and what’s on your plate, and it is associated with eating disorder development. Keep in mind that culture doesn’t just occur on TV, movies, social media, or glossy magazines—it’s everywhere, including conversations with friends and loved ones.
- You might be wondering, “Do diets cause eating disorders? The answer is no. They don’t directly cause them. But they are a major risk factor, especially dieting in adolescence or frequent dieting throughout life. Being in negative energy balance (aka a calorie deficit) can trigger an eating disorder in someone vulnerable.
Is recovery possible if you don’t know what caused it?
You might be wondering if you need to know the exact causes of yours or a loved one’s eating disorder to achieve recovery. The answer is no.
“Patients often want to figure out why,” Dr. Simmons says, “but I let them know that understanding patterns is helpful without needing to solve every piece of the past. Recovery isn’t dependent on having the perfect insight into what started everything.”
For example, family-based treatment (FBT) for eating disorders is agnostic. This means that it doesn’t focus on rooting out the cause. Yet it is one of the most effective approaches for eating disorder treatment.
She adds, “What matters more is restoring nourishment, rebuilding flexibility with food and movement, and strengthening relationships and support. Healing often comes from doing recovery, not just understanding it.”
The bottom line
I want to end on a hopeful note: eating disorder recovery is possible. I’m certainly living proof.
Although I now have a better understanding of why I developed disordered eating behaviors, the causes weren’t initially clear to me until more recently.But, even at the time, I was able to work with a wonderful therapist who helped me reframe my thought patterns related to food and exercise, using cognitive behavioral therapy (CBT).
Now exercise, specifically running, is something I love for how it makes me feel during and after, not a tool to punish my body for betraying me. And food is what provides me the nourishment to get out in the woods and on the trails or to fuel my brain while writing.
Recovery doesn’t mean perfection, and it looks different for everyone. I still experience triggers. But now I have the tools to recognize them and reframe my thoughts or ask for help when needed.
If you or a loved one are looking for recovery options, know that help is available. Talk with a trusted doctor or schedule a call with Equip to talk through your concerns and explore treatment options.
FAQ
What causes eating disorders?
Several factors can cause eating disorders. Researchers have landed on what’s called the biopsychosocial model to illustrate this. It means that a mix of biological, psychological, and social factors play a role.
Do you ever fully recover from an eating disorder?
Yes, you can fully recover from an eating disorder. However, even once recovered, triggers can still arise. Recovery teaches you the tools to manage these triggers to reduce your risk of relapse.
Can eating disorders be genetic?
Yes, family and twin studies show that inherited factors account for 28% to 84% of eating disorder risk.
Adamo, Kristi B., et al. “Appetite Sensations, Appetite Signaling Proteins, and Glucose in Obese Adolescents with Subclinical Binge Eating Disorder.” ISRN Obesity, vol. 2014, Mar. 2014, p. 312826.
Avena, Nicole M., and Miriam E. Bocarsly. “Dysregulation of Brain Reward Systems in Eating Disorders: Neurochemical Information from Animal Models of Binge Eating, Bulimia Nervosa, and Anorexia Nervosa.” Neuropharmacology, vol. 63, no. 1, Nov. 2011, p. 87.
Bany-Mohammed, Mo’men, et al. “Trauma, Stress, and Mental Health Outcomes.” Journal of Psychiatry and Psychiatric Disorders, vol. 9, no. 5, Sept. 2025, p. 276.
Balasundaram, Palanikumar, and Prathipa Santhanam. “Eating Disorders.” StatPearls, StatPearls Publishing, 2025.
Berge, Jerica M., et al. “Parent Conversations about Healthful Eating and Weight: Associations with Adolescent Disordered Eating Behaviors.” JAMA Pediatrics, vol. 167, no. 8, Aug. 2013, p. 746.
Bevilacqua, Arturo, et al. “Association of Serotonin Receptor Gene Polymorphisms with Anorexia Nervosa: A Systematic Review and Meta-Analysis.” Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity, vol. 29, no. 1, Apr. 2024, p. 31.
Brodrick, Brooks B., et al. “Structural Brain Differences in Recovering and Weight-Recovered Adult Outpatient Women with Anorexia Nervosa.” Journal of Eating Disorders, vol. 9, Sept. 2021, p. 108.
Broft, Allegra I., et al. “Bulimia Nervosa and Evidence for Striatal Dopamine Dysregulation: A Conceptual Review.” Physiology & Behavior, vol. 104, no. 1, Apr. 2011, p. 122.
Cristofori, Irene, et al. “Executive Functions.” Handbook of Clinical Neurology, vol. 163, 2019, pp. 197–219.
Cobbaert, Laurence, et al. “Neurodivergence, Intersectionality, and Eating Disorders: A Lived Experience-Led Narrative Review.” Journal of Eating Disorders, vol. 12, no. 1, Nov. 2024, p. 187.
Convertino, Alexandra D., et al. “Trauma Exposure and Eating Disorders: Results from a United States Nationally Representative Sample.” The International Journal of Eating Disorders, vol. 55, no. 8, June 2022, p. 1079.
Cuijpers, Pim, et al. “Absolute and Relative Outcomes of Cognitive Behavior Therapy for Eating Disorders in Adults: A Meta-Analysis.” Eating Disorders, vol. 33, no. 6, 2025, pp. 783–804.
Dell’Osso, Liliana, et al. “Historical Evolution of the Concept of Anorexia Nervosa and Relationships with Orthorexia Nervosa, Autism, and Obsessive-Compulsive Spectrum.” Neuropsychiatric Disease and Treatment, vol. 12, July 2016, pp. 1651–60.
Donato, Kevin, et al. “Gene Variants in Eating Disorders. Focus on Anorexia Nervosa, Bulimia Nervosa, and Binge-Eating Disorder.” Journal of Preventive Medicine and Hygiene, vol. 63, no. 2 Suppl 3, June 2022, pp. E297–305.
Esbenshade, Elizabeth, and Alexandra Venegas. “Biopsychosocial Review of Eating Disorders.” Open Journal of Psychiatry, vol. 14, no. 2, Feb. 2024, pp. 107–19.
Fitterman-Harris, Hannah F., et al. “Digital Mental Health Interventions: Differences in Diet Culture Intervention Framing.” International Journal of Environmental Research and Public Health, vol. 21, no. 1, Dec. 2023, p. 24.
Frank, Guido K. W. “The Perfect Storm - A Bio-Psycho-Social Risk Model for Developing and Maintaining Eating Disorders.” Frontiers in Behavioral Neuroscience, vol. 10, Mar. 2016, p. 44.
Hambleton, Ashlea, et al. “Psychiatric and Medical Comorbidities of Eating Disorders: Findings from a Rapid Review of the Literature.” Journal of Eating Disorders, vol. 10, Sept. 2022, p. 132.
Haleem, Darakhshan Jabeen. “Serotonin Neurotransmission in Anorexia Nervosa.” Behavioural Pharmacology, vol. 23, nos. 5–6, Sept. 2012, pp. 478–95. PubMed.
Ismaylova, Elmira, et al. “Brain Serotonin, Oxytocin, and Their Interaction: Relevance for Eating Disorders.” Journal of Psychopharmacology (Oxford, England), vol. 39, no. 3, Jan. 2025, p. 187.
Koller, Dora, et al. “Epidemiologic and Genetic Associations of Endometriosis With Depression, Anxiety, and Eating Disorders.” JAMA Network Open, vol. 6, no. 1, Jan. 2023, p. e2251214.
Li, Qingqing, et al. “Athlete Body Image and Eating Disorders: A Systematic Review of Their Association and Influencing Factors.” Nutrients, vol. 16, no. 16, Aug. 2024, p. 2686.
Suhag, Khushi, and Shyambabu Rauniyar. “Social Media Effects Regarding Eating Disorders and Body Image in Young Adolescents.” Cureus, vol. 16, no. 4, Apr. 2024, p. e58674.









