Anorexia Causes: How Biology, Environment, and Psychology Intersect


- Anorexia doesn’t have a single cause. It develops through a mix of biological vulnerability, psychological traits, and environmental influences that build over time.
- Risk factors, triggers, and reinforcing factors play different roles. Understanding the difference can help explain how anorexia takes hold without anyone or any particular thing being at fault.
- Dieting, illness, stress, or unintentional weight loss can act as a tipping point, especially for people who are already vulnerable.
- Anorexia can affect people of any body size, gender, or background. Weight stigma and praise for weight loss often delay recognition and treatment.

When people ask what caused my anorexia, I still hesitate—not because I don’t have ideas, but because the question assumes there’s a single, clear answer. There wasn’t. It developed gradually, shaped by a mix of biology, personality, and circumstances that I didn’t understand were causes of anorexia at the time.
That uncertainty is familiar to many parents and caregivers. A diagnosis of anorexia often comes with shock, fear, and guilt, along with questions like: Did I cause this? How did this happen? People experiencing anorexia may ask the same thing in a different way: Why me?
Here’s the most important thing to know upfront: anorexia does not have a single cause. It isn’t caused by bad parenting, vanity, or a lack of willpower. “Anorexia is a genetically loaded gun,” explains Michael Wetter, PsyD, ABPP, FAACO, a psychologist at UCLA Health and owner of Wetter Psychological Services. “Any number of environmental or societal factors can pull the trigger.”
That said, you don’t need to identify a specific cause to deserve help or begin recovery. Here, learn how anorexia can develop, what contributes to it, and what doesn’t, so you can move forward with clarity rather than blame.
The basics to know about anorexia
Anorexia nervosa is widely known, but it’s actually less common than many other eating disorder diagnoses. Estimates suggest it affects up to about 4% of women and 0.3% of men. It typically develops in kids and teens aged 11 to 19 years old, but can affect people at any stage of life, including young children and older adults.
At its core, anorexia involves ongoing food restriction and intense fear of weight gain or body changes. Because restriction can lead to malnutrition, anorexia is the most life-threatening eating disorder. It has one of the highest mortality rates of any psychiatric illness, with more than 5% of people dying within four years of diagnosis. Rates of anorexia have increased in recent years, especially among adolescent girls and young adult women.
But anorexia doesn’t look the same for everyone—symptoms can vary widely, and so can the factors that contribute to how the illness develops. Common signs of anorexia can include:
- Eating much less than the body needs or tightly restricting certain foods
- Feeling uncomfortable or avoiding eating in front of others
- Ritualized or obsessive eating behaviors
- Being highly focused on weight, shape, or body size
- Noticeable or ongoing weight loss
It’s also important to know that anorexia isn’t defined by your appearance. You don’t need to look underweight to be at risk or need help. People of any body size can experience anorexia and its physical and mental effects. In fact, there’s a specific diagnosis for people who meet all the criteria for anorexia except for low body weight, known as atypical anorexia.
What causes anorexia?
“Anorexia is a complex mental health condition,” says Sonya Elefante, LCSW, LCADC, a therapist at Equip. “There are several factors that increase the likelihood of developing AN, though none are predictive on their own. These risk factors span biological, psychological, social, and cultural domains.”
It’s helpful to think of anorexia as a process rather than a formula. There isn’t a set equation where certain traits or experiences automatically lead to the disorder. Some people have underlying vulnerabilities and need only a small trigger for symptoms to emerge. Others may have fewer risk factors but experience a cluster of stressors that shifts their relationship with food and their body, explains Wetter.
Clinicians often group these influences into three categories. These categories overlap and interact, and their balance looks different for every person:
- Risk factors that increase vulnerability
- Triggers that mark the start of restrictive behaviors
- Reinforcing factors that keep anorexia going once it begins
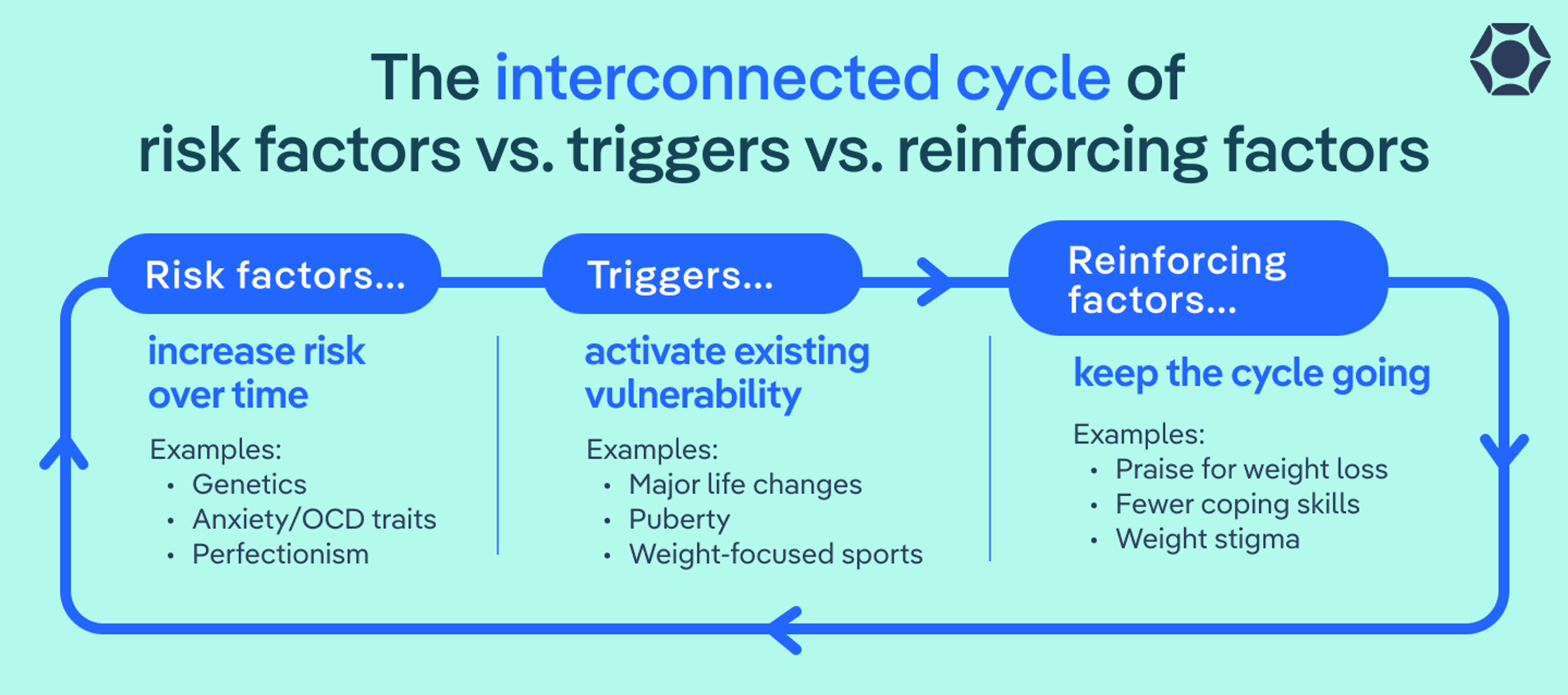
Risk Factors vs. Triggers vs. Reinforcing Factors
Risk factors increase vulnerability over time
- Genetics
- Brain chemistry
- Perfectionism
- Anxiety or OCD traits
- Neurodivergence
- Gender-related stress
Triggers activate existing vulnerability
- Dieting or restriction
- Illness or weight loss
- Stress or life changes
- Puberty
- Trauma
- Weight-focused sports
- Cultural body pressure
Reinforcing factors keep the cycle going
- Restriction provides relief from hard emotions
- Brain changes from underfueling
- Praise for weight loss
- Weight stigma
- Fewer coping skills
What are the risk factors for anorexia?
Risk factors are not causes of eating disorders. Having one—or even several—doesn’t mean someone will develop anorexia. They simply increase a person’s vulnerability, especially when multiple factors overlap. Often, these vulnerabilities have been there for a long time, even before anyone notices changes in eating, which can make anorexia feel like it came out of nowhere.
Genetics
Research consistently shows that your genetics are part of the story. If you have a close family member with anorexia or another eating disorder, your own risk is higher, says Elefante. “This increased risk likely reflects a combination of genetic influences and environmental factors such as learned behaviors,” she explains.
This vulnerability often overlaps with family histories of anxiety, depression, or obsessive-compulsive traits, which commonly show up alongside anorexia, adds Wetter.
Neurobiology
For some people, the way their brain is wired can make them more vulnerable to anorexia, says Wetter. In fact, research has found differences in brain chemistry and in the systems that handle reward, fear, and impulse control among people who develop the illness.
What this can mean in real life is that food restriction may feel unusually calming or relieving, especially during times of stress. Signals like hunger, fullness, or fatigue may also feel muted or confusing, making it easier for restriction to continue without setting off internal alarms. These are brain-based differences, not choices or personal failures.
Psychological traits
According to Wetter, certain personality traits and thinking patterns also show up frequently before anorexia develops, such as:
- Perfectionism
- Rigid thinking
- Feeling uncomfortable with uncertainty and change
Wetter adds that difficulty tolerating distress and managing strong emotions, particularly during stressful or overwhelming periods, often overlaps with anorexia, too. For some, restriction can start to feel like a way to cope—even though it ultimately makes things harder.
Neurodivergence
Neurodivergent people, including those with autism or ADHD, may face additional challenges that increase vulnerability. Sensory sensitivities, strong preferences for routine, or intense focus on rules can make eating more complicated, even before any disordered behaviors appear.
For example, certain food textures, unpredictability around meals, or changes in routine can be genuinely distressing. These traits don’t cause anorexia—but in the right (or wrong) circumstances, they can make someone more vulnerable.
Sex and gender identity
Anorexia affects people of all genders. While it’s more commonly diagnosed in women and girls, boys, men, and transgender and nonbinary individuals are likely underdiagnosed and may face more barriers to care, says Elefante. Transgender and gender-diverse youth, in particular, may experience added vulnerability related to body distress, gender dysphoria, minority stress, or lack of affirming support.
Taken together, these risk factors help explain why anorexia can develop in people who seem outwardly “fine,” and why there’s never a single, simple explanation. Most importantly, they reinforce a truth many families and individuals need to hear: Vulnerability is not a failure, and it’s not something anyone chooses.
What are common triggers that can lead to anorexia?
Triggers don’t cause anorexia on their own. Instead, they can be what “turns on” an eating disorder when biological and psychological risk factors are already present, explains Wetter. Often, triggers are ordinary life experiences—things that wouldn’t cause an eating disorder in most people, but can tip the balance for someone who’s already vulnerable.
“It is important to note that while these circumstances may act as a catalyst or accelerate progression, they do not cause the eating disorder,” adds Elefante.
Dieting, restriction, and negative energy balance
Dieting and intentional restriction are among the most common triggers for anorexia, says Wetter. Most people aren’t trying to develop an eating disorder—they’re trying to be “healthier,” or under-eating due to a busy schedule, or responding to subtle pressure around weight or food. That’s how it started for me.
Here’s how this happens: restriction can lead to negative energy balance (also known as a calories deficit), meaning the body is burning more fuel than it’s getting. If you’re vulnerable to anorexia, this state can change how the brain functions, increasing anxiety around food while also making restriction feel relieving or calming. Over time, that relief can reinforce the behavior and make it harder to stop.
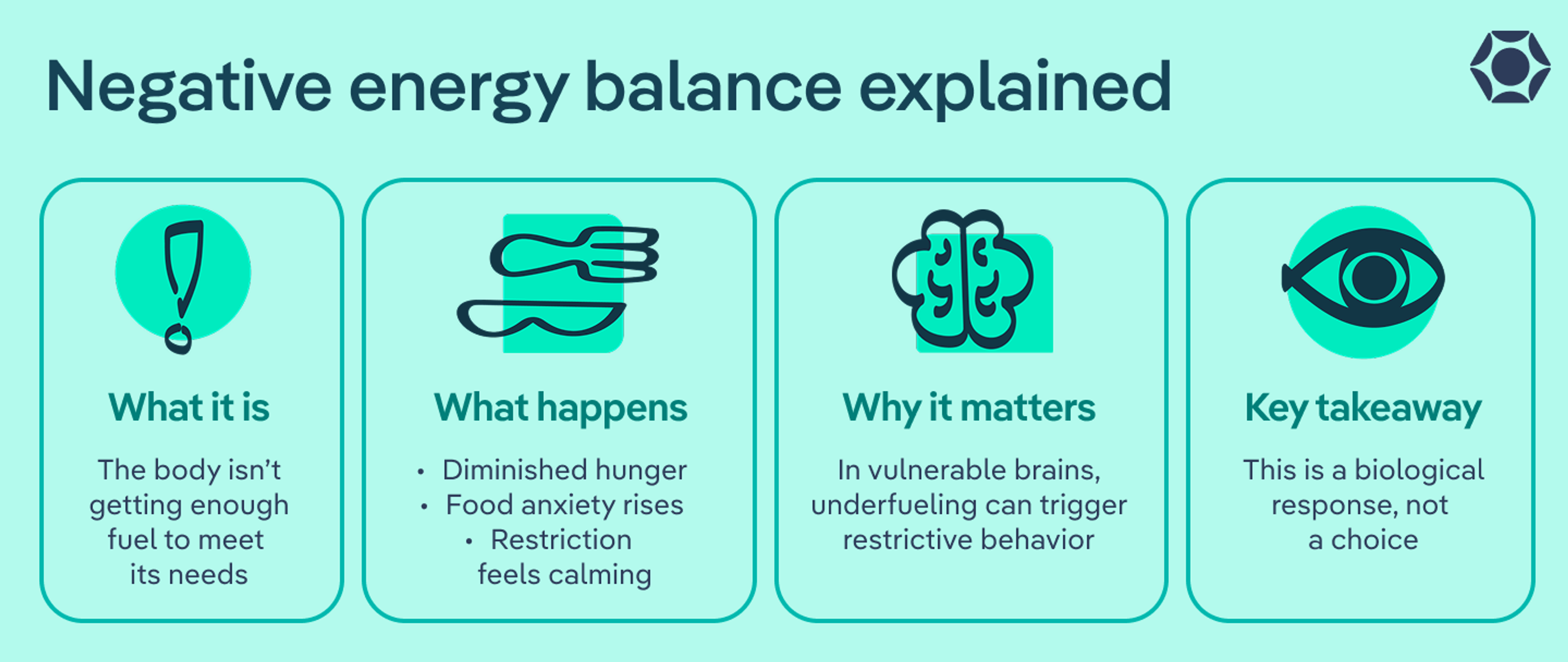
Negative Energy Balance, Explained
What it is: The body isn’t getting enough fuel to meet its needs.
What happens:
- Hunger signals get quieter
- Anxiety around food increases
- Restriction can feel calming or relieving
Why it matters: In vulnerable brains, underfueling can “flip a switch,” reinforcing restrictive behaviors even when no harm is intended.
Key takeaway: This is a biological response, not a choice.
Puberty
Puberty is a period of intense physical, emotional, and neurological change. Hormonal shifts, rapid growth, and body changes can increase vulnerability, especially for kids and teens who are sensitive to control, perfectionism, or body discomfort. During this stage, even small changes in eating or activity can have outsized effects on the brain and body.
Trauma, stress, and life transitions
According to Elefante, restriction can become a coping mechanism when life feels unpredictable or emotionally overwhelming. Traumatic or stressful events that can contribute to this include:
- Bullying
- Grief
- Abuse
- Illness
- Family conflict
- Divorce
- Moving
- Starting a new school or job
Media and cultural messages
Cultural pressure around body size, health, and appearance can also act as a trigger, especially if you’re already vulnerable to the condition, says Wetter. This can look like:
- Exposure to unrealistic body “ideals” or diet culture
- “Clean eating” messages
- Constant comparison on social media
Altogether, these factors can quietly shape beliefs about worth, control, and success. While these messages don’t cause anorexia by themselves, they can normalize restriction and make early symptoms harder to recognize.
Athletic and professional pressures
Certain sports and performance-driven environments place extra emphasis on body size, weight, or appearance. In these settings, early restriction may be praised or encouraged, which can delay concern and reinforce eating disorders in athletes. While eating disorders can affect athletes in any sport, the activities most commonly associated with anorexia include::
- Gymnastics
- Ballet
- Figure skating
- Cheerleading
- Wrestling
- Distance running
- Bodybuilding
- Weight-class sports
What factors reinforce anorexia?
“The same factors that increase the risk of developing AN can also reinforce symptoms,” says Elefante. Changes in the brain, body, and environment can also quickly turn early symptoms into a self-perpetuating cycle.
Restriction as a coping mechanism
In the short term, restriction can feel like it helps, according to Wetter. For some people, eating less brings a sense of control during chaotic or stressful periods. For others, it numbs difficult emotions or quiets anxiety. That relief is temporary, but it’s powerful.
Over time, as restriction becomes a go-to coping strategy, healthier ways of managing stress or emotions get crowded out. The brain learns, incorrectly, that not eating is what keeps things manageable.
Malnutrition affects the brain
Malnutrition doesn’t just affect the body—it significantly affects the brain. One of the clearest examples of this is the Minnesota Starvation Study, which found that prolonged energy restriction leads to increased anxiety, obsessive and rigid thinking, and preoccupation with food.
Put simply, starvation alters brain chemistry in ways that can reinforce anorexia, says Wetter. Prolonged restriction can heighten fear around eating, contribute to rigid thinking, and make it harder to think clearly or change course. In this state, continuing to restrict can actually feel psychologically rewarding, even as physical health deteriorates.
It’s important to remember this isn’t a character flaw—it’s a predictable biological response to underfueling.
Social reinforcement and weight stigma
External feedback can also reinforce anorexia, often unintentionally. In a culture that praises weight loss, early changes in eating or body size may be met with compliments or encouragement, says Wetter. I experienced this firsthand—at first, the attention felt positive, even affirming.
Those responses can quietly reinforce restriction and make it harder for anyone to recognize what’s really happening. When weight loss is automatically treated as a good thing, early signs of distress or malnutrition are easier to miss (or are brushed off altogether). This is especially true for people in large bodies, who are more likely to have their symptoms dismissed or praised, allowing anorexia to progress further before it’s named or treated.
What doesn’t cause anorexia?
When anorexia shows up, it’s common for people—especially parents and caregivers—to blame themselves or others for things that do not actually cause anorexia, including:
- Bad parenting: Anorexia isn’t the result of being too strict, too permissive, too focused on food, or not focused enough. Parents do not cause anorexia, even when symptoms first appear at home.
- Vanity: Anorexia isn’t caused by a desire to be thin, a phase, or a bid for control or approval, says Wetter. People don’t choose anorexia, and they don’t stay in it because they enjoy it.
- Lack of willpower or motivation: Anorexia is a serious mental illness that changes how the brain and body function. Once restriction takes hold, willpower alone isn’t enough to undo it, he says.
- A single comment, meal, or mistake: Even well-intended remarks about food, bodies, or health do not cause anorexia on their own. The illness develops through a much broader and more complex process.
“Anorexia is not a lifestyle choice [or] moral failing,” says Wetter. “People do not choose to develop anorexia, nor can they 'snap out of it' through willpower alone.”
These misconceptions can carry a real emotional cost. Blame and guilt often slow down help-seeking and add unnecessary distress. Understanding what doesn’t cause anorexia helps shift the focus back to support, care, and healing.
What Doesn’t Cause Anorexia
- Bad parenting
- Vanity
- Desire to be thin
- Lack of willpower
- A phase
- A single comment or meal
Anorexia is a serious illness, not a personal failure or parenting mistake.
The bottom line
There’s never one cause of anorexia, and it doesn’t follow a single path. Instead, it develops through a mix of biological vulnerability, psychological traits, and life experiences that interact over time. For many families and individuals, that complexity is exactly what makes the illness so confusing.
What matters most is this: No one causes anorexia, and you don’t need to understand why it started in order to deserve help. You don’t have to wait until things get worse. You don’t have to be certain. And you don’t have to carry guilt as proof that you care.
Anorexia is serious, but it is also treatable. With the right support, nourishment, and evidence-based care, recovery is possible. Reaching out sooner rather than later can make a meaningful difference, for both the person experiencing anorexia and the people who love them. If you’re here wondering whether it’s time to ask for help, that question alone is often reason enough to start the conversation.
FAQ
How does anorexia develop?
Anorexia usually develops over time. It often begins when underlying vulnerabilities—like genetics, anxiety, perfectionism, or how the brain responds to stress—intersect with something that changes eating, such as dieting, illness, stress, or a major life shift. Once restriction begins, underfueling can change how the brain works, making the behaviors feel harder to stop. That’s why anorexia can feel like it took over, even if it didn’t begin that way.
Can anorexia develop without dieting or trying to lose weight?
Yes. Dieting is common, but it’s not the only path. Anorexia can also begin after unintentional weight loss from illness, increased activity, chronic stress, or skipped meals during busy or overwhelming periods. In some cases, restriction starts as a way to cope or feel in control, not to lose weight. What matters isn’t the original intention, but what happens when the body isn’t getting enough fuel.
Do you need to know what caused anorexia to treat it?
No. You don’t need a clear explanation or a single “cause” to start treatment or recover. Many people never land on a neat answer, and that’s completely okay. Treatment focuses on nourishment, support, and breaking the patterns that keep anorexia going, not on figuring out exactly how it started.
Allam, Alexandra et al. “Body Image, Disordered Eating, and Eating Disorders in Gender Diverse Youth.” Current pediatrics reports vol. 13,1 (2025): 10.1007/s40124-025-00341-1. doi:10.1007/s40124-025-00341-1
Barakat, Sarah et al. “Risk factors for eating disorders: findings from a rapid review.” Journal of eating disorders vol. 11,1 8. 17 Jan. 2023, doi:10.1186/s40337-022-00717-4
Borowiec, Joanna et al. “Eating disorder risk in adolescent and adult female athletes: the role of body satisfaction, sport type, BMI, level of competition, and training background.” BMC sports science, medicine & rehabilitation vol. 15,1 91. 25 Jul. 2023, doi:10.1186/s13102-023-00683-7
Donato, Kevin et al. “Gene variants in eating disorders. Focus on anorexia nervosa, bulimia nervosa, and binge-eating disorder.” Journal of preventive medicine and hygiene vol. 63,2 Suppl 3 E297-E305. 17 Oct. 2022, doi:10.15167/2421-4248/jpmh2022.63.2S3.2772
Frank, Guido K W et al. “Association of Brain Reward Response With Body Mass Index and Ventral Striatal-Hypothalamic Circuitry Among Young Women With Eating Disorders.” JAMA psychiatry vol. 78,10 (2021): 1123-1133. doi:10.1001/jamapsychiatry.2021.1580
Grilo, Carlos M, and Tomoko Udo. “Examining the significance of age of onset in persons with lifetime anorexia nervosa: Comparing child, adolescent, and emerging adult onsets in nationally representative U.S. study.” The International journal of eating disorders vol. 54,9 (2021): 1632-1640. doi:10.1002/eat.23580
Moore, Christine A, and Brooke R Bokor. “Anorexia Nervosa.” National Library of Medicine, StatPearls Publishing, 2023, www.ncbi.nlm.nih.gov/books/NBK459148/.
Nagy, Hassan et al. “A Clinical Overview of Anorexia Nervosa and Overcoming Treatment Resistance.” Avicenna journal of medicine vol. 13,1 3-14. 21 Dec. 2022, doi:10.1055/s-0042-1758859
Norton, Bethany et al. “Overlap of eating disorders and neurodivergence: the role of inhibitory control.” BMC psychiatry vol. 24,1 454. 18 Jun. 2024, doi:10.1186/s12888-024-05837-6
Rousseau, Léna et al. “Burden of negative energy balance in anorexia nervosa: Role of circadian rhythm, mitochondrial dynamics, microbiota-gut-brain axis and their interactions.” Clinical nutrition (Edinburgh, Scotland) vol. 52 (2025): 27-45. doi:10.1016/j.clnu.2025.07.002
Suhag, Khushi, and Shyambabu Rauniyar. “Social Media Effects Regarding Eating Disorders and Body Image in Young Adolescents.” Cureus vol. 16,4 e58674. 21 Apr. 2024, doi:10.7759/cureus.58674
van Eeden, Annelies E et al. “Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa.” Current opinion in psychiatry vol. 34,6 (2021): 515-524. doi:10.1097/YCO.0000000000000739
Westmoreland, Patricia et al. “Causes of death in patients with a history of severe anorexia nervosa.” Journal of eating disorders vol. 10,1 200. 24 Dec. 2022, doi:10.1186/s40337-022-00716-5









